

This month’s issue of JAMA addresses the question “Does this patient have a blunt intra-abdominal injury?” as part of the always-popular Rational Clinical Examination series.
The systematic review of the literature summarizes the accuracy of findings for your blunt trauma patient in diagnosing intra-abdominal injuries. Specifically, likelihood ratios (LR) are summarized. These LRs can be used to plot on the Bayes nomogram below. You draw a straight line connecting your pretest probability and the LR. This yields your posttest probability.

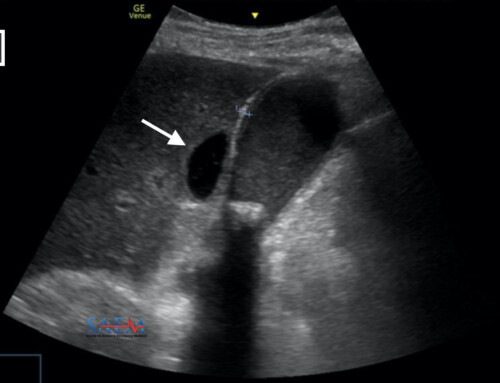
The most predictive positive LR include: Abdominal rebound tenderness, a “seat belt sign”, ED hypotension, hematocrit < 30%, AST or ALT > 130, urine with > 25 RBCs, base deficit < -6 mEq/L, and a positive FAST ultrasound.
The trouble is that the absence of these findings aren’t as helpful in ruling-out injury, with negative LR’s very close to 1.0. The two exceptions are base deficit and FAST ultrasound with a negative LR of 0.12 and 0.26, respectively.
Adapted from [1]
Go to ALiEM (PV) Cards for more resources.
I find it interesting that there are studies on hepatic transaminase levels. Anyone else getting these in their trauma patients? I traditionally don’t. Many of our patients have a history of hepatitis C and underlying alcoholic hepatitis. If suspicious for blunt abdominal trauma, we just get the CT.
Reference
- Nishijima D, Simel D, Wisner D, Holmes J. Does this adult patient have a blunt intra-abdominal injury? JAMA. 2012;307(14):1517-1527. [PubMed]

Professor and Digital Innovation Lab Director
Department of Emergency Medicine
University of California, San Francisco
@M_Lin
Latest posts by Michelle Lin, MD (see all)
- EM Match Advice 42: Mid Interview Season Check-In - January 5, 2024
- EM Match Advice 41: The 2024 ERAS Application – New and Improved - July 24, 2023
- EM Match Advice 40: Program Directors Reflect on the 2023 Match - May 17, 2023


{kind=link}
{kind=link}
{kind=link}