
 The detection rate of sternal fractures following motor vehicle collisions and blunt trauma to the chest and abdomen has increased over the past decade. The reason for this increase is most likely from the use of seat belts and better imaging modalities such as computed tomography (CT) in trauma patients. I can recall as a resident being told that any patient with a sternal fracture should be admitted to trauma because of the high likelihood of blunt cardiac injury and high mortality rate associated with this injury, but is this always true?
The detection rate of sternal fractures following motor vehicle collisions and blunt trauma to the chest and abdomen has increased over the past decade. The reason for this increase is most likely from the use of seat belts and better imaging modalities such as computed tomography (CT) in trauma patients. I can recall as a resident being told that any patient with a sternal fracture should be admitted to trauma because of the high likelihood of blunt cardiac injury and high mortality rate associated with this injury, but is this always true?
In isolated sternal fractures, what is the rate of cardiac complications and mortality?
| Study | Year Published | Number of Patients with Isolated Sternal Fracture | Cardiac Complications | Deaths |
| Athanassiadi K et al | 2002 | 67 | 3 (pericarditis 1; hemo-pneumothorax 1; hemomediastinum 1) | None |
| Wiener et al | 2001 | 50 (22 with isolated sternal fracture) | 11 (benign pericardial effusion 7; arrhythmia 3; ST-T abnormality 1) | None |
| Sadaba JR et al | 2000 | 37 | 1 (atrial fibrillation) | None |
| Peek GJ et al | 1995 | 117 | None | None |
| Heyes FLP et al | 1993 | 55 total patients (Unknown how many isolated sternal fractures) | None | None |
| Brookes JG et al | 1993 | 123 | None | None |
| Wright SW et al | 1993 | 31 | None | None |
| Johnson I et al | 1992 | 103 total patients (Unknown how many isolated sternal fractures | None | None |
| Jackson M et al | 1992 | 104 | None | None |
| Breederveld RS et al | 1988 | 52 | None | None |
Does the location of the sternal fracture make a difference? 1
- 58 patients with sternal fracture
- Isolated sternal fracture in 9% of these patients
- Predominant fracture location was the manubrium (36.2%)
- 76.2% of patients with manubrium fractures ended up in ICU
- 23.8% of patients with manubrium fractures died (largest mortality rate)
- Most commonly associated injuries: rib fractures (63%) and spinal fractures (57%)
- Most common causes of sternal fractures were frontal car collision and fall from greater than 5 meters
- Conclusion: Fractures of the manubrium are associated with other injuries and have a higher mortality rates
Are there guidelines for screening of blunt cardiac injury (BCI)? 2
- Eastern Association for the Surgery of Trauma practice management guideline
- 35 studies reviewed
- Great blunt cardiac injury algorithm from The Trauma Professional’s Blog
- Another blunt cardiac injury algorithm from EM Clinics of North America paper (2012) summarized as PV card 3
- Note that in both algorithms above, a troponin level is only warranted if there is an abnormal ECG.
Level 1 Recommendations
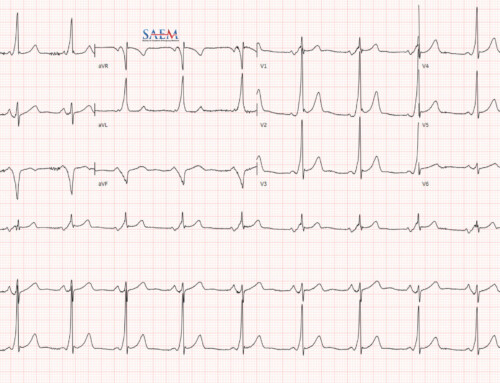
- ECG should be performed on all patients in whom BCI is suspected
Level 2 Recommendations
- If ECG reveals a new abnormality (arrhythmia, ST changes, ischemia, heart block, and unexplained ST changes), patient should be admitted for telemetry
- If normal ECG and normal troponin, blunt cardiac injury is ruled out
- Hemodynamically unstable patients, or persistent new arrhythmia, echocardiogram should be obtained
- Presence of sternal fracture alone does not predict presence of blunt cardiac injury in setting of normal ECG and cardiac enzymes
- CPK and CK-MB should not be performed in predicting blunt cardiac injury
Level 3 Recommendations
- Elderly patients with known CAD, hemodynamically unstable patients, and patients with abnormal screening ECG can safely undergo emergent surgery with appropriate monitoring
- Cardiac computed tomography or magnetic resonance imaging can be used to differentiate acute myocardial infarction form blunt cardiac injury in trauma patients with abnormal ECG, cardiac enzymes, and/or abnormal echocardiogram
What is the role of troponin in BCI?
Per the EAST guidelines:
“ECG remains the most commonly recommended tool for initial diagnosis of BCI. Less clear is the role that troponin should play in addition to ECG in the diagnostic workup, although it seems that this may allow for safe discharge or admission to a regular ward. A normal ECG result has an excellent NPV, in most studies being greater than 95%. Some studies, however, indicate that the addition of troponin I will increase the NPV to 100%, which could potentially decrease overall costs should that allow for more discharges and avoidance of intensive care unit stay.”
Take Home Messages
- Diagnosis of sternal fracture does require a high index of suspicion for associated injuries (especially fracture of the manubrium).
- When isolated, sternal fracture can be surprisingly benign, but screening ECG should be obtained.
- Abnormal ECG or cardiac enzymes with an isolated sternal fracture requires observation for possible blunt cardiac injury.
- Bottom Line: Isolated sternal fractures, not involving the manubrium with normal ECG and cardiac enzymes (if ordered) can be safely discharged home.

Salim Rezaie, MD
Latest posts by Salim Rezaie, MD (see all)
- Blast From the Past: Occult Sepsis, Lactic Acid, and Mortality - June 29, 2015
- Therapeutic Hypothermia After Pediatric Cardiac Arrest Out-of-Hospital (THAPCA-OH) Trial - May 25, 2015
- ADJUST-PE Study: ALiEM-Annals of EM Journal Club - August 25, 2014


{kind=link}
{kind=link}
{kind=link}