
SplintER Series: My Knee, Again!

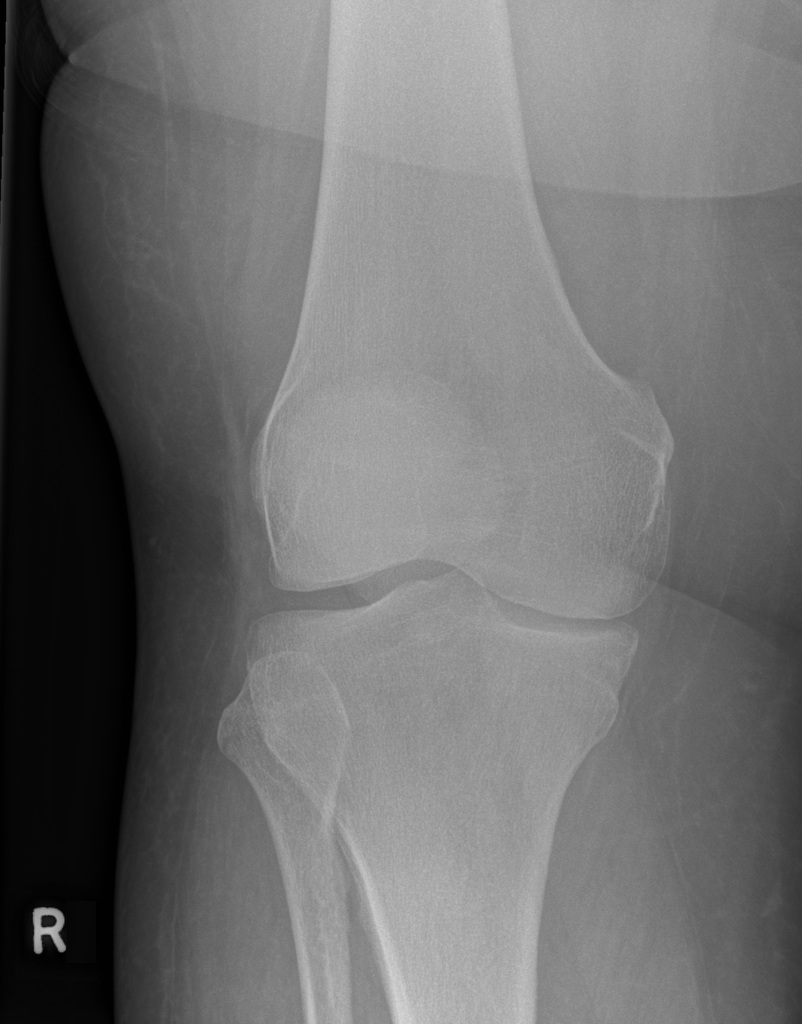
A 61-year-old F presents to the ED from the orthopedic clinic with acute right knee pain. She endorses that while a physical exam was being performed, she had sudden onset knee pain. Denies any trauma to the knee, radiation of pain, numbness, tingling, or swelling. The above knee radiographs were obtained (Images courtesy of John Kiel, DO).




{kind=link}