
EM ReSCu Peds 12: Penetrating Trauma
Brief Narrative Description of Case
This scenario takes place at a Level 1 trauma center. The patient is 4 year old and was an accidental casualty in a drive-by shooting. He has a gunshot wound to his right torso causing hemodynamic instability. On primary survey, learners will ideally recognize that the patient is having respiratory distress and perform needle decompression and place a chest tube. The patient will also need emergent airway management with adjuncts, bag valve mask, and/or intubation. The patient has an intra-abdominal hemorrhage, requiring aggressive fluid resuscitation and blood transfusion (initiation of institutional massive transfusion protocol). The learner should communicate to the parent(s) the interventions that were performed and provide a final disposition to the operating room for definitive management.

Primary Learning Objectives
At the end of this simulation, participants should be able to:
- Demonstrate the evaluation of a pediatric patient with penetrating trauma using a standard systematic approach
(application) - Construct and implement initial medical management plan for a child with a penetrating trauma (application)
- Perform fluid resuscitation for shock including institutional protocol for blood transfusion (application)
- Demonstrate airway management of a sick child using appropriate adjuncts, bag valve mask, and/or endotracheal intubation (application)
- Demonstrate needle decompression, pediatric chest tube placement, and tube size selection (application)
- Demonstrate focused history taking from a caregiver (application)
- Explain diagnosis and management to caregivers (synthesis)
- Demonstrate teamwork and closed loop communication (application)
- Develop a plan for transfer to a trauma center for definitive management (synthesis)
Critical Actions
- Team lead assigns roles
- Obtain focused history from emergency medical services (EMS) and additional SAMPLE history from parents
- Place patient on monitor and obtain initial vital signs
- Obtain vascular access (intravenous or intraosseous)
- Perform primary survey and identify tension pneumothorax
- Manage pediatric airway
- Employ proper use of airway adjuncts (may include effective bag-mask ventilation (BMV), nasopharyngeal airway, oropharyngeal airway, laryngeal mask airway, jaw thrust, shoulder roll)
- Obtain a definitive airway (endotracheal intubation or surgical airway)
- Perform proper needle decompression and chest tube placement with appropriate size selection
- Perform E-FAST exam and identify intra-abdominal hemorrhage
- Perform adequate intravenous fluid resuscitation for hypovolemic shock
- Initiate massive transfusion protocol
- Complete secondary survey
- Call pediatric trauma service for disposition to operating room, and notify Pediatric Intensive Care Unit or other appropriate higher level of care
- Communicate effectively and compassionately with parents of a sick child
- Disposition patient to the operating room
Case Creators
Authors
- Daphne Morrison Ponce, MD, LCDR(MC), USN
- Kelly Murphy, MD, MS
Editors
- Manu Madhok, MD
- Rebekah Burns, MD
- Sean Stuart, DO, LCDR, MC, USN, FAAEM, FACEP, FAWM
- Whitney Minnock, MD
- Nicholas Koch, MD
Updated August 19, 2020
Setup
Chief complaint: Gun shot wound to right abdomen
Patient age: 4 years old
Weight: 18 kg
Recommended Supplies
- Manikin: Trauma child
- Moulage: Gun shot wound (GSW) to the right abdomen/thorax (entrance wound at right subcostal margin, exit wound on right mid back), blood stained clothes
- Resources: Pediatric Advanced Life Support (PALS) cards and/or length-based tape (e.g., Broselow Tape)
- Manikin set up:
- Ability to needle decompress the right chest and place a chest tube. Can be set up separate from manikin on skills trainer, depending on available simulation equipment available. If only adult trauma manikin, consider increasing the age of the child (e.g., 10 years old, 30 kg)
- Extremities available for peripheral IV placement attempts and intraosseous (IO) device access
- Equipment:
- PALS cart to include airway equipment
- Nasopharyngeal airways (NPA)
- Laryngeal mask airways (LMA)
- Oropharyngeal airways (OPA)
- Cuffed endotracheal tubes
- Laryngoscope blades and handles
- Bag mask ventilation (BMV) with appropriate sized masks
- Ventilator
- Needles for pneumothorax decompression (14g and 16g peripheral IVs)
- Chest tube set ups
- Tube thoracostomy 18/20/22 Fr
- Percutaneous chest tube kits
- Pleuravac
- IV supplies and tubing
- IO supplies
- Video laryngoscope (optional)
- PALS cart to include airway equipment
- Medications: Rapid sequence intubation (etomidate, ketamine, succinylcholine, rocuronium), sedation/analgesia (fentanyl, morphine, versed), blood products (uncrossed trauma cooler), tranexamic acid, cefazolin, Tdap immunization, cardiac arrest medications (code cart – epinephrine, atropine, calcium chloride, amiodarone, lidocaine, dextrose 50%), IV fluids
Supporting Files
- Ultrasound: FAST images which shows fluid in the abdomen and absent lung sliding on the right
- Chest radiograph (CXR) showing appropriate chest tube placement
- Lab results with blood gas showing mild metabolic acidosis, low/normal hemoglobin/hematocrit, and mild transaminitis. Urinalysis with hematuria.
Participants/Roles
- Learners
- Team leader
- Airway manager / respiratory therapist ᴑ Medication preparer
- Medication giver
- Recorder (optional)
- Pharmacist (optional)
- ED technician (optional)
- Embedded participant
- Parent(s) of the patient – provides history of event and SAMPLE history. Asks about pain medicine for the patient, if not given. If the patient goes to the operating room without informing you, ask what’s going on and what’s going to happen.
- Nurse – provides exam findings, if asked, for parts of the exam difficult to simulate. Can decide if initial peripheral intravenous lines are successful or if want to push learner to intraosseous access.
- Consultants – Surgical fellow/attending – can be phantom and provide phone consult if needed.
Prerequisite Knowledge
- Faculty
- PALS protocols
- General knowledge of emergency medicine
- Simulation implementation and debriefing experience
- Emergency medicine residents
- Any stage of training (preferably PGY- 2 or higher for team lead; recommended after Pediatric intensive care unit rotation)
- Completed PALS certification
- Trauma assessment and management training, such as Advanced Trauma Life Support (ATLS)
- Familiarity with pediatric airway management
- Criteria for institutional trauma team activation (EM1)
- Knowledge of institutional massive transfusion protocol (EM1)
- Skills training on needle decompression and chest tube placement
- Training on E-FAST performance
Recommended to Review Prior to Session
- Intubation and chest tube placement for pediatric patients
Case Alternatives
- The patient could go into pulseless electrical activity (PEA) if chest decompression is not done within 2 minutes of presentation.
- The patient remains hemodynamically unstable until the chest tube is placed and a massive transfusion protocol (MTP) initiated.
- Incorporate transfer concerns and consideration of limited resources, if setting changed to a non-trauma center or non- pediatric hospital.
- Can increase case difficulty by making patient have a difficult airway due to blood or general poor visibility.
Milestones
PC1. Emergency Stabilization
PC2. Performance of Focused History & Physical Exam
PC3. Diagnostic Studies
PC4. Differential Diagnoses and Management
PC5. Pharmacotherapy
PC7. Disposition
PC8. Task-Switching
PC9. General Approach to Procedures
PC10. Airway Management
PC11. Anesthesia and Acute Pain Management
PC12. Goal-directed Focused Ultrasound (Diagnostic/Procedural)
PC15. Medical Knowledge
PC22. Patient Centered Communication
PC23. Team Management
Resources
- McFadyen JG, Ramaiah R, Bhananker SM, et al. Initial Assessment and management of Pediatric Trauma Patients. Int J Crit Illn Inj Sci; 2:121-127. PMID 23181205
- Dudley NC, Hansen KW, Furnival RA, et al. The Effect of Family Presence on the Efficiency of Pediatric Trauma Resuscitations., Ann Emerg Med; 53:777-84. PMID 19013688
- Sobolewski B. Do we need to perform a digital rectal exam in injured children? PEM Cincinnati blog. Published May 2016. Accessed June 2020.
- Fox SM. Pediatric Trauma Pitfalls. PEM Morsels. Published June 2019. Accessed June 2020.
- Nickson C. Trauma! Penetrating Abdominal Injury. Life in the Fast Lane. Published Feb 2019. Accessed June 2020.
- Interfacility Transfer Toolkit for the Pediatric Patient, M.a.C.H.B. Health Resources and Services Administration, EMSC (EMSC) Program, Editor. 2018. p. 1-42.
- Bhananker S, McFadyen J, Ramaiah R. Initial assessment and management of pediatric trauma patients. International Journal of Critical Illness and Injury Science. 2012;2: 121-127.
- Committee On Pediatric Emergency Medicine, C.O.I., et al., Management of Pediatric Trauma. Pediatrics, 2016. 138(2).
- Cotton BA, Nance ML. Penetrating trauma in children. Semin Pediatr Surg, 2004. 13(2): 87-97.
- Dudley NC, Hansen KW, Furnival RA, Donaldson AE, Van Wagenen KL, Scaife ER. The effect of family presence on the efficiency of pediatric trauma resuscitations. Ann Emerg Med. 2009; 53(6):777-84.e3.
- Hansen M, Meckler G, oʼBrien K, et al. PediatricAirway Management and Prehospital Patient Safety: Results
of a National Delphi Survey by the Children’s Safety Initiative-Emergency Medical Services for Children. Pediatr Emerg Care. 2016;32(9):603-607. - Nakayama DK, Gardner MJ, Rowe MI. Emergency endotracheal intubation in pediatric trauma. Ann Surg. 1990;211(2):218-223.
- Rotondo M, Cribari C, Smith R. Resources for Optimal Care of the Injured Patient. Committee on Trauma. 2014, Chicago, IL: American College of Surgeons. 1-215.
- Shroyer MC, Griffin RL, Mortellaro VE, Russell RT. Massive transfusion in pediatric trauma: analysis of the National Trauma Databank. The Journal of Surgical Research. 2017 Feb;208:166-172.
- Starnes AB, Oluborode B, Knoles C, Burns B, McGinnis H, Stewart K. Direct Air Versus Ground Transport Predictors for Rural Pediatric Trauma. Air Med J. 2018;37(3):165 -169.
| ITEM | FINDING |
|---|---|
| Overall Appearance | 4-year-old male with eyes closed, whimpering, and with rapid shallow respirations. Blood stained clothes greater on the right side. |
| HPI | Instructor: “You receive a call from EMS that a patient is being brought in after a shooting at a nearby shopping mall. EMS was not able to establish vascular access, and they are now at your front doors. The parent accompanies the patient.”
Parent: “We were in line to get Auntie Annie’s pretzel when someone just opened fire. I think it was gang related. I tried to pull him out of harm’s way, but I was not fast enough. As soon as I saw he was hit, I called 911. Is he going to die?” If the learner asks for it: No additional information given. The learner must interview parent and EMS for below information. |
| Past Medical/Surgical History | No past medical history. Parents have limited access to health care and have not completed the immunization schedule. |
| Medications | None |
| Allergies | Apples and pears; no known drug allergies |
| Family History | No history of bleeding disorders |
| Social History |
|
Primary Survey (A-B)
Start through needle compression and intubation
Critical Actions
- Team lead assigns roles
- Place patient on monitor and obtain full set of vital signs
- Obtain vascular access and order labs
- Perform primary survey
- Identify tension pneumothorax
- Needle decompression
- Manage pediatric airway (can be done in next step)
- Employ proper use of airway adjuncts (may include effective BMV, NPA, OPA, LMA, jaw thrust, shoulder roll)
- Obtain a definitive airway (endotracheal intubation or surgical airway)
- Initiate volume resuscitation (blood or saline)
Physical Exam
| ITEM | FINDING |
|---|---|
| Vital Signs | T: 37.1oC, HR: 160, BP: 68/48, RR: 36, SpO2: 85% |
| Airway | No airway obstruction, no pooling of secretions, no stridor. If asked, the trachea is deviated to the left. |
| Breathing | Agonal and shallow breathing at rate of 36. Absent breath sounds on the right. Asymmetric chest rise. |
| Circulation | Palpable pulses in all extremities, 4-second capillary refill, and cool extremities. |
| Disability | Dextrose – Point of care glucose 105 mg/dL
Glasgow Coma Scale (GCS) = 8
Alternative rating system:
|
| Exposure | No additional wounds identified. No area of massive hemorrhage posteriorly. |
Instructor Notes: Changes and Case Branch Points
| INTERVENTION / TIME POINT | CHANGE IN CASE | ADDITIONAL INFORMATION |
|---|---|---|
| Needle decompression not performed with primary survey or attempt to confirm with chest radiograph (CXR) | Patient will arrest into pulseless electrical activity (PEA) | PEA arrest (electrical rate 53 without a pulse, blood pressure or pulse oximetry reading). Return of spontaneous circulation (ROSC) when needle decompression performed. |
| Access can be IV or IO. Labs can be obtained from either source. The examiner can choose to push to IO, if desired. | If the facilitator desires IO placement, the nurse can state, “The IV blew” or “I’m unable to place the IV.” | |
| Needle decompression/ chest tube placement attempted | Parent angrily asks: “Why are you stabbing my child with a needle? Aren’t you supposed to do no harm!?” | Parent continues to ask questions until the learner addresses him and tactfully asks him to watch but not interfere with medical care. Can call social work/ chaplain for support. |
| Appropriate needle decompression performed | Whoosh of air, breathing improves, BP improves to 72/50 mmHg, HR unchanged, saturations increase to 92%. | Oxygen saturation improves; however, BP will not fully correct until the patient receives blood products (in the next stage). |
| Rapid sequence intubation (RSI) without initiation of fluid resuscitation, or if no volume resuscitation given in first 5 minutes | BP decreases to 60/40 mmHg. | If the case progresses without the learner addressing the hypotension, can give cue with a question from the nurse, such as “The patient’s pressure is still really low.” |
| Intubation attempt without RSI medications (laryngoscope blade placed in oropharynx before medications are called for) | The patient vomits. The SpO2 decreases to 80%. The heart rate decreases to 80. | Alternative: PEA arrest and after 1 round of CPR, the patient has ROSC. During PEA, the heart rate is sinus at 53 bpm without a pulse, blood pressure, or readable pulse oximeter reading. The airway can either be secured during or after after the code. |
| Intubation with RSI medications | The RR changes to the bagged rate. The SpO2 is 95%. Proceed to Stage 2. | |
| Sedation orders not placed after intubation | Parent and nurse state that the patient seems uncomfortable after the intubation. | Satisfied with bolus or drip sedation |
| Learners ask for advanced imaging such as a CT scan | Nurse states “I don’t feel comfortable taking him to the CT scanner with that blood pressure.” | The patient should go to the operating room without advanced imaging. |
Completion of Primary Survey
Completion of Primary Survey:Needle decompression and intubation through completion of primary survey (A through E), massive transfusion protocol, and chest tube placement
Critical Actions
- Obtain focused history from EMS, additional SAMPLE history from parents
- Manage pediatric airway (if not done in Stage 1)
- Employ proper use of airway adjuncts (may include effective BMV, NPA, OPA, LMA, jaw thrust, shoulder roll)
- Obtain a definitive airway (endotracheal intubation or surgical airway)
- Complete secondary survey
- Perform proper chest tube placement with appropriate size selection (if not done in Stage 1)
- Reassess volume resuscitation and initiate massive transfusion protocol (MTP) per institutional protocol and consider TXA
- Call pediatric trauma service for disposition to OR, and notify PICU (Institution appropriate trauma team activation)
- Perform FAST exam and identify intra-abdominal hemorrhage
* Unbolded items may be excluded depending on local practices and norms
Physical Exam
| ITEM | FINDING |
|---|---|
| Vital Signs | T: 37.3oC, HR: 140, BP: 72/54, RR: 16-20, SpO2:98% |
| General | Ill-appearing with blood-stained clothes. Eyes closed. |
| HEENT | 4 mm pupils are equal and reactive. No head or neck trauma. No hemotympanum. Face stable. Oropharynx clear, no blood. No scalp hematomas. |
| Neck | No posterior midline tenderness; no stepoffs, deformities, or crepitus |
| Lungs | Fast but shallow respirations. Absent breath sounds on the right. Single bullet hole to the right torso. E-FAST with no lung sliding on the right. |
| Cardiovascular | Regular rhythm, tachycardic. No murmurs. Palpable pulses with delayed (>4 sec) cap refill. Cool extremities. |
| Abdomen | No hepatomegaly. E-FAST with fluid in the right upper quadrant (Morrison’s pouch). No bruising. No distention. Abdominal wound present with oozing. |
| Neurological | GCS 8 (eyes open to painful stimuli, moans incoherently, withdraws to pain). Moves all extremities. Normal tone. |
| Skin | Cool, clammy, diaphoretic |
| Back | Normal rectal tone and gluteal squeeze. Non-tender spine with no stepoffs, deformities, or crepitus |
| Extremities | Soft compartments, no deformity |
| Exam changes |
|
Instructor Notes: Changes and Case Branch Points
| INTERVENTION / TIME POINT | CHANGE IN CASE | ADDITIONAL INFORMATION |
|---|---|---|
| Initiation of blood products | BP improves to 80/60 mmHg | Should follow institutional protocol to activate massive transfusion protocol. |
| Resident calls for incorrect size of chest tube | Nurse asks, “Doctor, are you sure about that tube size?” | Chest tube size chart on Broselow tape. |
| Chest tube placed | Air leak present in the chamber; go to Stage 3. | Nurse will report 50 mL of frank blood and air from chest tube, if asked. |
| Chest radiograph not ordered | x-ray tech comes in and asks, “Hey did you want an x-ray on this kid?” or trauma surgeon can request a CXR to confirm tube positioning. | Chest tube and endotracheal tube (ETT) in appropriate position. No retained ballistic fragments. Pneumothorax decompressed. |
| Massive transfusion not initiated (by minute 10 of simulation time) or positive FAST images misinterpreted/not obtained | The patient continues to get more tachycardic (180 beats per minute) and hypotensive (60/40 mmHg). | PEA arrest if not recognized. After x2 doses of epinephrine and blood transfusion will get ROSC. |
| Needs airway secured for anticipated clinical course | Nurse can ask, “He doesn’t seem to be protecting his airway, should we intubate him before moving to the OR?” |
Reassessment and Disposition
Chest tube placed, airway secured, blood products through discussion with surgeon
Critical Actions
- Consult (Pediatric) Trauma surgery (confederate) and give recommendations for urgent ex-laparotomy
- Activate appropriate level trauma (if not already done)
- Communicate effectively and compassionately with parents of a sick child
- Discuss care with parents
* Unbolded items may be excluded depending on local practices and norms
Physical Exam
| ITEM | FINDING |
|---|---|
| Vital Signs | T: 37.3oC, HR: 140, BP: 80/60, RR: 18, SpO2: 98% |
| Exam Changes |
|
Instructor Notes: Changes and Case Branch Points
| INTERVENTION / TIME POINT | CHANGE IN CASE | ADDITIONAL INFORMATION |
|---|---|---|
| Embedded participant (surgeon or nurse) is called before a tetanus shot is updated | The surgeon asks “Did he get all his vaccinations… including the one for tetanus?” or the nurse prompts to ask about tetanus status. | Case proceeds to the OR either way. This is a point for feedback and the learner should consider. |
| Learner does not address parent about disposition to OR | Parent asks, “What is going on? Where are you taking my son? Is he going to live?” | Case proceeds after parent updated on plan and disposition |
Demonstrate the evaluation of a pediatric patient with penetrating trauma using a standard systematic approach (application)
- Evaluation of traumatic injuries follows a standardized approach taught in Advanced Trauma Life Support (ATLS)
- Evaluation begins with addressing any life-threats identified in the ABCs. This is followed by a head to toe exam known as the secondary survey. This includes continued reassessment and a return to ABCs as the clinical condition changes.
- The E-FAST exam typically occurs during or after the secondary survey.
Construct and implement initial medical management plan for a child with a penetrating trauma (application)
- Penetrating trauma accounts for 10-20% of pediatric trauma admissions. Of these injuries, gunshot wounds are the most common mechanism. [Cotton B, Nance M. Penetrating Trauma in Children. Seminars in Ped Surg. 2004 May;13(2): 87-97. PMID 15362278]
- Firearm injuries have the highest fatality rate for all mechanisms and all age groups. Firearm injuries double at age 12 and increase until age 22. Prior to age 12, firearms account for 2% of trauma and 15% of traumatic mortality. [National Trauma Data Bank 2016 Annual Report. Accessed June 2020.]
- Penetrating trauma often requires surgical intervention. The assessment and evaluation of a child with penetrating trauma should focus on stabilization and getting surgical services available.
- Immediate stabilization can include airway management, needle decompression/chest tube placement, volume resuscitation, tourniquet application, fracture immobilization, or other similar procedures.
- This approach is similar for adult patients, but varies primarily in medication dosing and equipment sizing.
Perform fluid resuscitation for shock including institutional protocol for blood transfusion (application)
- Massive transfusion protocols vary between institutions, but typically should be implemented when there is an ongoing or anticipated large volume transfusion need.
- Tranexamic acid (TxA) should be administered within 3 hours of injury.
Demonstrate airway management of a sick child using appropriate adjuncts, BMV, and/or endotracheal intubation (application)
- Airway management is a critical component of pediatric resuscitation, especially in trauma patients. This is not limited to endotracheal (ETT), and should also include your adjuncts of BMV and OPA/NPA. The goal of ETT is to ensure optimal gas exchange. Most common indications for ETT in a trauma patient: Coma, shock, apnea, airway obstruction
- Common airway complications: Right mainstem intubation, esophageal intubation, massive aspiration, unilateral or bilateral vocal cord paralysis, subglottic stenosis, failure to adequately preoxygenate, and extubation during transport
Demonstrate needle decompression, pediatric chest tube placement, and tube size selection (application)
- Background on pneumothorax and hemothorax:
- Accumulation of air and blood (respectively) in the space between the visceral and parietal pleura of the hemithorax can impair oxygenation, ventilation and hemodynamics.
- In traumatic hemothorax, >15 mL/kg blood at time of insertion or >3-4 mL/kg/hr is an indication for surgical intervention. This is similar to adults (>1500 mL at insertion or ongoing >150 mL/hr).
- Etiologies may include traumatic, spontaneous or iatrogenic.
- Signs, symptoms, and exam findings vary, but can include being asymptomatic, dyspnea, chest pain, asymmetric chest rise, tracheal deviation, hypoxia, and hypotension.
- Diagnosis and management:
- A pneumothorax can quickly be confirmed with ultrasound or chest x-ray.In the appropriate clinical setting, needle decompression should be performed immediately.
- Needle decompression can be performed in the midclavicular line, 2nd intercostal space or the anterior mid-axillary line in the 5th intercostal space.
- Lin, M. “Trick of the Trade: Don’t miss the pneumothorax in needle thoracostomy”. Academic Life in Emergency Medicine. Published Oct 2012. Accessed June 2020.
- Needle decompression is a stabilizing procedure and should be followed by placement of a chest tube or surgical intervention.
- Chest tube placement: Similar to adults, a chest tube should be placed in the 5th intercostal space at the midaxillary line. [Busti AJ, Hinson J. “Chest Tube Thoracostomy”. Evidence-Based Medicine Consult. Published Sept 2015. Accessed June 2020.]
- Chest tube size
- Use Broselow tape
- Calculate size using formula
- 4 x ETT = maximum chest tube size (e.g., used for hemothorax)
Demonstrate focused history taking from a caregiver (application)
- Components of history taking: Past medical history, surgical history, family history, medications, allergies, social history, vaccination history
- SAMPLE mnemonic (S – signs and symptoms; A – allergies; M – medications; P – pertinent past medical history; L – last oral intake; E – events leading up to presentation) is helpful to quickly obtain necessary information.
- For this scenario, obtaining a quick history of pertinent medical problems, allergies, and events is critical.
Explain diagnosis and management to caregivers (synthesis)

Use a teach-back approach
Develop a plan for transfer to a trauma center for definitive management (synthesis)
- The American College of Surgeons (ACS) accredits pediatric and adult trauma centers. Your local EMS system likely has protocols to transfer directly to a trauma capable facility. However, non- pediatric trauma centers will be needed to stabilize and transfer pediatric patients.
- It is important to consider your facility’s pediatric readiness to provide initial stabilization and transfer to a variety of both medical and trauma pediatric patients requiring a higher level of care.
- Consider ground versus air transport depending on the patient’s condition, medical needs during transport, risk for decompensation, and distance to travel. Consider utilizing available critical care or pediatric specific transport teams
Demonstrate teamwork and closed loop communication (application)
Teams may use different frameworks to improve team dynamics and communication. Below are a few definitions that may be helpful to discuss, adapted from the AHRQ TeamSTEPPS Pocket Guide.
- Brief: Short session prior to start of encounter to share the plan, discuss team formation, assign roles and responsibilities, establish expectations and climate, anticipate outcomes and likely contingencies
- Huddle: Ad hoc team discussion to re-establish Situation Awareness; designed to reinforce plans already in place and assess the need to adjust the plan
- Callout: A strategy used to communicate critical information during an emergent event. Helps the team prepare for vital next steps in patient care. (Example: Leader- “Airway status?”; Surveying provider- “Airway clear”; Leader- “Breath sounds?”; Surveying provider- “Breath sounds decreased on right”)
- Check-back: A closed-loop communication strategy that requires a verification of information ensuring that information conveyed by the sender is understood by the receiver as intended. The sender initiates the message; the receiver accepts it and restates the message. In return, the sender verifies that the re-statement of the original message is correct or amends if not. (Example: Leader- “Give diphenhydramine 25 mg IV push”; Med Prep- “Diphenhydramine 25 mg IV push”; Leader- “That’s correct”)
- SBAR: A framework for team members to structure information when communicating to one another.
- S = Situation (What is going on with the patient?)
- B = Background (What is the clinical background or context?)
- A = Assessment (What do I think the problem is?)
- R = Recommendation (What would I do to correct it?)
- Situation monitoring: The process of continually scanning and assessing a situation to gain and maintain an understanding of what is going on around you.
- Situation awareness: The state of “knowing what’s going on around you.”
- Shared mental model: Result of each team member maintaining situation awareness and ensures that all team members are “on the same page.” An organizing knowledge structure of relevant facts and relationships about a task or situation that are commonly held by team members.
- STEP: A tool for monitoring situations during complex situations. A systematic method to review Status of patient, Team members’ performance and status, Environment, and Progress towards goal.
- Cross-monitoring: A harm error reduction strategy that involves 1. Monitoring actions of other team members 2. Providing a safety net within the team. 3. Ensuring that mistakes or oversights are caught quickly and easily. 4. “Watching each other’s back.”
- CUS: Signal phrases that denote “I am Concerned,” “I am Uncomfortable,” and “This is a Safety Issue.” When spoken, all team members should understand clearly not only the issue but also the magnitude of the issue.

E-FAST Ultrasound Images: RUQ View

E-FAST Ultrasound Images: LUQ View

E-FAST Ultrasound Images: Pelvic View

E-FAST Ultrasound Images: Subxiphoid View of the Heart

E-FAST Ultrasound Images: Parasternal Long View of the Heart
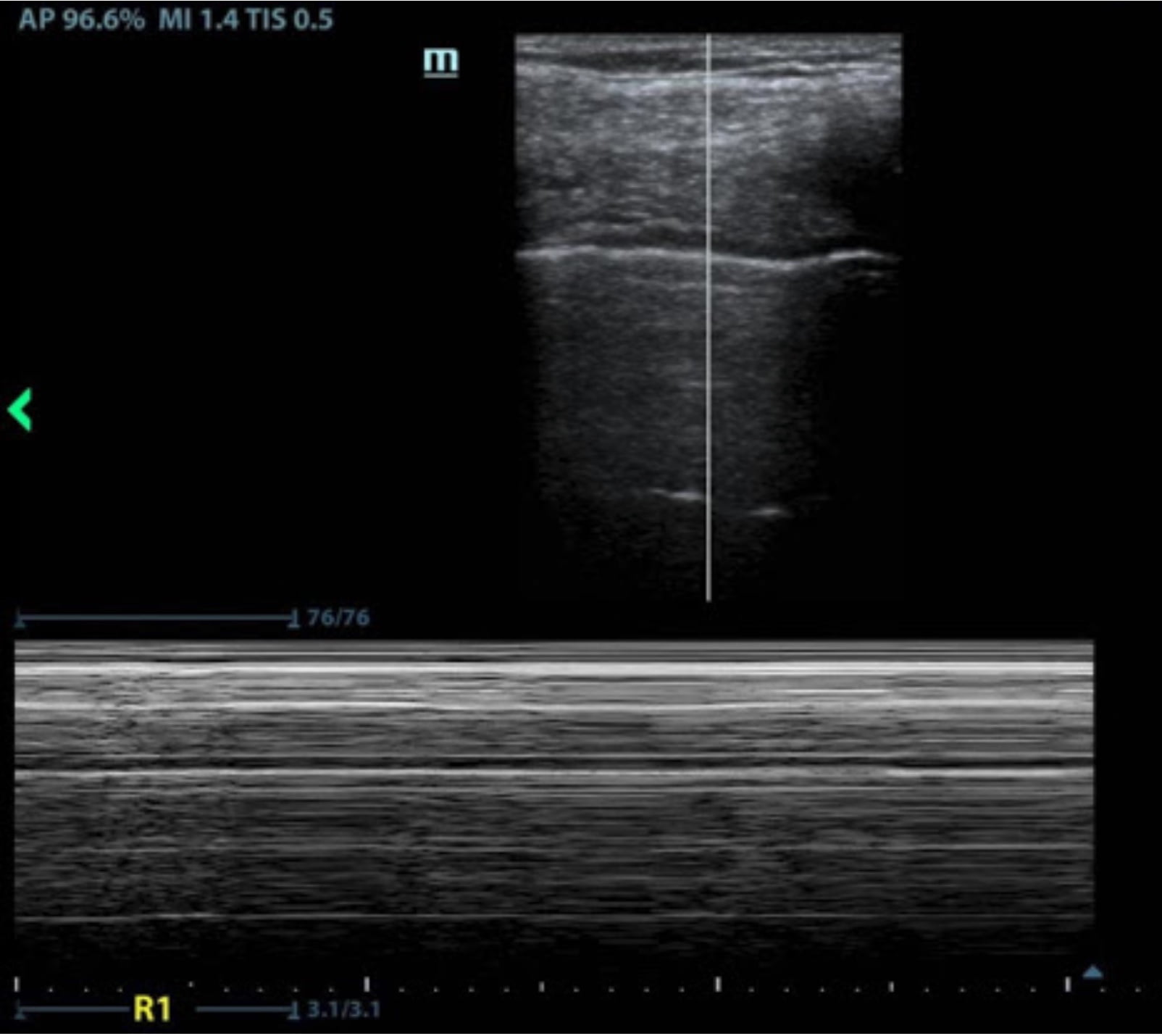
E-FAST Ultrasound Images: Right Lung View in M-Mode

E-FAST Ultrasound Images: Left Lung View in M-Mode

Chest X-ray
Download Case 12 supporting files
Notes:
- E-FAST Interpretation: Images from Dr. Daphne Morrison Ponce
- RUQ View: No free fluid
- LUQ View: No free fluid
- Pelvis View: Free fluid in pelvis
- Subxiphoid View: No pericardial effusion
- Parasternal Long View: No pericardial effusion
- Right Lung View: Suggestive of a pneumothorax given “bar code” appearance in M-mode
- Lung Lung View: No pneumothorax given “seashore” appearance in M-mode
- Chest X-ray Interpretation: CXR with chest tube in posterior apex with lung re-expansion. Image from Dr. Daphne Morrison Ponce.
For the embedded participant playing the patient’s parent
Case Background Information
The patient is your 4-year-old son. You were at the local shopping mall when there was an active shooter. He was injured on his right side. He is bleeding from the injury. He is moaning and having difficulty breathing. He needs emergent blood transfusion and a chest tube to remove air from around his lung. You are very worried about him and feeling guilty for being at the location of the shooting.
Who are the Learners?
Emergency medicine residents
They should inform you briefly of what they are doing and speak with you more in-depth prior to moving your son to a different location in the hospital.
Standardized Patient Information
Your 4-year old son was shot on the right side when there was an active shooter at the shopping mall. You are very worried about him because he’s not talking and interacting normally. Additionally, you’re feeling guilty for being in the location where there was an active shooter. You feel responsible for not protecting him. The medical team should acknowledge your concerns and provide basic information upon arrival (e.g., “he’s very sick, we’re going to take care of him”, “we need to put a breathing tube in place, we will talk more in a moment”). In the beginning of the case, there will be many critical medical actions.
If the team plans to transfer your son to the operating room, ICU, another hospital location, or other area outside the Emergency Department without updating you on his condition and plan of care, you should become more insistent with your questions.
Patient Information
(Please remember not to offer any of this information, but when asked please respond while remaining in character.)
- CHIEF COMPLAINT (your response to open-ended questions such as “what’s going on?” or “what can we do for you? Or “what happened?”): “Somebody shot my son.”
- AGE: 4 years old
- ADDITIONAL HISTORY: “We were in line to get Auntie Annie’s pretzel when someone just opened fire. I think it was gang related. I tried to pull him out of harm’s way, but I was not fast enough. As soon as I saw he was hit I called 911. Is he going to die?” “He’s getting sleepier and not talking to me.”
- PAST MEDICAL HISTORY: Healthy, partially vaccinated due to difficulty with access to care
- SOCIAL HISTORY: Lives at home with mother, father, and older brother. Smoking outside the house only. No access to firearms at home. Pet dog.
- FAMILY HISTORY: No history of bleeding disorders
- PAST SURGICAL HISTORY: None
- MEDICATIONS: None
- ALLERGIES: Apples and pears. No known drug allergies.
- IMMUNIZATIONS: Vaccinated initially. 1-year shots were given late because we couldn’t get appointment with his PCP. Thinks he caught up on all vaccines except the 4-year-old shots.
Potential Dialogue
IMPORTANT: Do not offer unsolicited information. Please allow the learners to ask questions. Do not offer information unless they ask you.
Continue to express concern about your son without being obstructive.
Things you could say without being asked:
- “Is he going to be okay? Is he in pain? I should have moved him out of the way.”
Things you might say triggered by events in the scenario:
| EVENT | YOUR POTENTIAL RESPONSE |
|---|---|
| After your child is intubated and/or has a chest tube place | “Is he in pain? Why is he breathing like that?” |
| When your child is given a blood transfusion | “Is that safe? Why does he need blood?” |
| If your child is being moved to OR/ICU | “Where are you taking my son?” |
The learners enter the room to find a trauma patient altered and in respiratory distress. They immediately start their primary survey while delegating team members to place the patient on a bedside monitor, order for IV access and supplemental O2, and obtain a brief history.
- Learners immediately recognize that the patient is hypoxic and hypotensive with fast and shallow breathing, and that there are no breath sounds on the right. Immediate needle decompression leads to temporary resolution of a tension pneumothorax.
- If IV access is difficult to obtain, the learners should proceed to IO access. Labs are obtained, prioritizing type and crossmatch.
- Supplemental oxygen is provided, and an IV fluid bolus is ordered. The patient remains altered with GCS 8 and is intubated for airway protection.
- The E-FAST exam is positive for intraperitoneal blood and lack of lung sliding (if performed prior to chest tube/decompression).
- The patient’s respiratory distress has improved; however, hypotension is refractory to IV fluids until massive transfusion protocol is initiated and going.
- The team lead decides on operative management, informs the parent of the care plan, and consults the pediatric trauma surgery service for emergent exploratory laparotomy.
Anticipated Management Mistakes
- Difficulty with bedside monitors: Learners may be unfamiliar with equipment and fail to correctly place monitor leads, apply an inappropriate cuff sizing for a pediatric patient, or fail to hook the manikin up to the defibrillator if the patient goes into PEA. The facilitator can cue learners to use a Broselow tape/bag/cart or other resource to select the correct equipment (depending on what is available in your simulation center). If an inappropriate cuff is selected, you can report that the blood pressure doesn’t result and have the nurse suggest the cuff is incorrectly sized.
- Failure to immediately recognize the need for needle decompression: If this is not done within the first 3 minutes from the start of the case, the patient will go into circulatory collapse and PEA. The PALS algorithm is started.
- Failure to recognize the need for intubation: The patient has no obvious airway obstruction, but his diminished GCS is a concern for airway protection. The patient may start coughing/gagging on secretions if this is not addressed by the end of Stage 2.
- Ignoring family in the room: Learners will likely forget that the family is in the room if they stay quiet or get annoyed with them if they are in the way too much. They will have to balance informing the parent what is going on while asking him to not be a hindrance to medical care.
- Failure to resuscitate with blood products: Should initiate and follow massive transfusion protocol for your local institution. If no protocol is available, recommend administration of tranexamic acid and balanced transfusion (including packed red blood cells, platelets, and fresh frozen plasma). The instructor can prompt learners by calling from the blood bank and asking about the anticipated amount of products needed or ask if they want the protocol initiated.
- Difficulty with access: After brief (no more than two) attempts at peripheral IV lines, learners should proceed to IO access. The nurse or instructor can say “I don’t see any available veins, and we’ve already tried twice. Is there anything else we could do?” to prompt IO placement if needed.
- Recognition of need for operative management: Residents should not pursue advanced imaging or admission to a critical care setting. They should advocate for their patient if the surgeon is resistant to going to the operating room.
Feedback
Please complete our brief survey describing your experience.
Learner (scan or click on QR code)

Facilitator (click or scan QR code)


Professor and Digital Innovation Lab Director
Department of Emergency Medicine
University of California, San Francisco
@M_Lin