

An 18-year-old male presents to the Emergency Department (ED) with right shoulder pain after wrestling with his brother. He heard a “pop,” and has been having pain along his right clavicle and shoulder since. He is unable to move his right shoulder. No numbness, tingling, or weakness in his arm or hand. No dysphagia, stridor, or shortness of breath. No medical or surgical history. He has no history of shoulder dislocation or fractures.


Vitals: HR 71; BP 139/77; RR 18; O2 sat 98% on RA
General: Uncomfortable appearing young man with his right arm held in adduction and internal rotation.
Respiratory: Clear breath sounds without stridor or shortness of breath.
CV: Heart is regular rate and rhythm without murmur, rub or gallop. Radial pulses are 2+ bilaterally, with brisk capillary refill.
MSK: Right shoulder without gross deformity. Right sternoclavicular joint is boggy, tender to palpation, and asymmetric when compared to the left. Limited active range of motion due to pain.
Neuro: Grip strength is 5/5 bilaterally, with intact motor and sensation demonstrated in the radial, median and ulnar distributions.
Shoulder and clavicular x-ray: No fracture or dislocation.
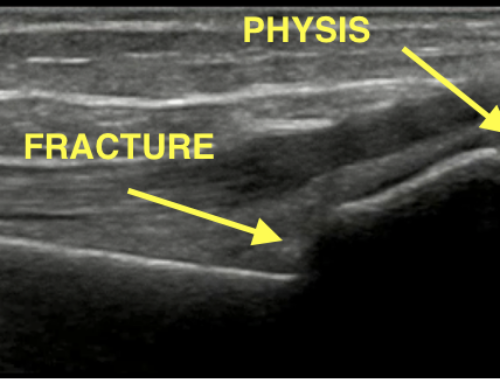
Point-of-care ultrasound: Clavicle (blue circle) posterior to the sternum (red square) at the sternoclavicular joint.
This is a posterior sternoclavicular dislocation. These dislocations are rare and are often the result of indirect lateral shoulder compression. It takes a high level of suspicion to diagnose as the physical exam and initial x-ray may be unrevealing. These patients require admission with emergent orthopedic consultation as there is a 30% chance of developing life-threatening complications due to damage of underlying structures including the trachea, esophagus, innominate artery and vein, and thoracic duct. Closed reduction in the operating room (OR) is typically the first line of treatment, with open reduction and internal fixation with cardiothoracic surgery consult available as the secondary treatment option.
CT with contrast is the imaging modality of choice, showing the sternoclavicular relationship in detail and allowing for evaluation of the underlying vascular and mediastinal structures. If unavailable, an oblique “serendipity view” x-ray may allow for better evaluation of the sternoclavicular joint than a standard shoulder or clavicle series. Additionally, point-of-care ultrasound can be an imaging modality that allows for quick and reliable bedside evaluation and diagnosis of sternoclavicular dislocation.
Take-Home Points
- Consider posterior sternoclavicular dislocation for those with traumatic shoulder or clavicular pain, particularly when the initial x-ray is unrevealing.
- Posterior sternoclavicular dislocation can have subtle exam findings that are easily missed if a high level of suspicion is not maintained.
- Posterior sternoclavicular dislocations can result in damage to underlying structures and require emergent orthopedic consultation for reduction in the OR with cardiothoracic backup available.
- Bengtzen RR, Petering RC.Point-of-Care Ultrasound Diagnosis of Posterior Sternoclavicular Joint Dislocation. The Journal of Emergency Medicine. (2017) Volume 52,(4) 513-515. https://https://doi.org/10.1016/j.jemermed.2016.11.001.
- Deren ME, Behrens SB, Vopat BG, Blaine TA. Posterior sternoclavicular dislocations: a brief review and technique for closed management of a rare but serious injury. Orthop Rev (Pavia). 2014 Mar 12;6(1):5245. doi: 10.4081/or.2014.5245. PMID: 24744842; PMCID: PMC3980158.
- Grantier III RL, Craddock P. Recanting Impressions: Posterior Sternoclavicular Joint Dislocation. EMResident, Published 2018 June 6.
- Roepke C, Kleiner M, Jhun P, Bright A, Herbert M. Chest Pain Bounce-Back: Posterior Sternoclavicular Dislocation. Ann Emerg Med. 2015 Nov;66(5):559-61. doi: 10.1016/j.annemergmed.2015.09.015. PMID: 26497437.

Sarah Shaver, MD
Department of Emergency Medicine
University of Texas Southwestern
Latest posts by Sarah Shaver, MD (see all)
- SAEM Clinical Images Series: My Shoulder Hurts - March 20, 2023

Craig Brockman, MD
Department of Emergency Medicine
University of Texas Southwestern
Latest posts by Craig Brockman, MD (see all)
- SAEM Clinical Images Series: Green Foot - March 13, 2026
- SAEM Clinical Images Series: Back Lesion - February 2, 2024
- SAEM Clinical Images Series: My Shoulder Hurts - March 20, 2023


{kind=link}
{kind=link}
{kind=link}