

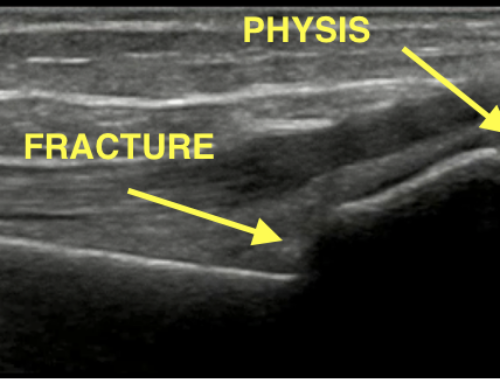
Image 1. Case courtesy of Radswiki, Radiopaedia.org
A 26 year-old male presents with new medial right knee pain after twisting his knee playing soccer 3 weeks ago. His initial pain has since resolved.
What is your diagnosis? What examination findings should you expect? What associated diagnoses should you assess for? What is your management in the emergency department?
Pellegrini-Stieda syndrome or disease. The lesion seen at the medial femoral condyle is known as a Pellegrini-Stieda sign – a calcification which was historically pathognomonic for a previous injury of the medial collateral ligament (MCL). Recent studies, however, have demonstrated that old injuries to the medial gastrocnemius, adductor magnus, and medial patellofemoral ligament can be associated with this calcification [1].
- Pearl: Pellegrini-Stieda can be seen in patients without knee trauma. It can also be seen in patients with spinal cord injury or traumatic brain injury. This is thought to be more associated with heterotopic ossification or myositis ossificans [2].
- Decreased range of motion
- Tenderness to palpation of the medial femoral condyle
- Pain with valgus stress
- Laxity with valgus stress
- Anterior cruciate ligament tear
- Posterior cruciate ligament tear
- Lateral collateral ligament tear
- Meniscal injury
- Neurovascular injury resulting from an unstable knee

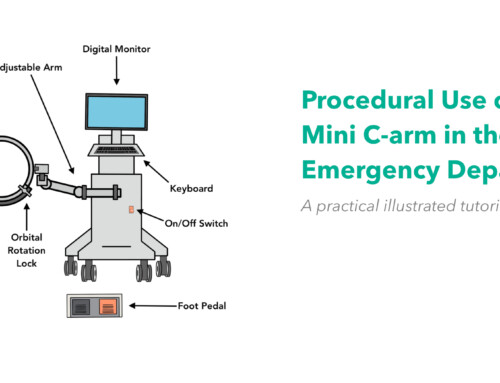
Image 2. Knee Ligaments, courtesy of BruceBlaus
- Pearl: A reverse Segond fracture is an avulsion of the MCL insertion on the medial tibia, as opposed to Pelligrini-Stieda, which is an ossification of the MCL at the medial femoral condyle.
- Pearl: Remember to perform the 2-minute knee exam to assess for other ligamentous injuries.
Pain control with anti-inflammatories. Consider crutches to allow for appropriate ambulation. Follow up with sports medicine and physical therapy.
- Pearl: As an outpatient, the patient will receive physical therapy. Corticosteroid injections are considered. Severe, refractory cases may require surgical excision [2].
- Pearl: This lesion can be confused for a fracture if incidentally noted on a knee x-ray. Be sure to clarify history of any recent injury – it could be a new avulsion fracture of the medial femoral condyle (Stieda fracture). Normally, patients with Pellegrini-Stieda disease can be discharged without immobilization, but if there is concern for acute fracture by history, consider offering a hinged knee immobilizer or other functional bracing.
References:
- Mendes, L., Pretterklieber, M., Cho, J., Garcia, G., Resnick, D. and Chung, C. (2006). Pellegrini–Stieda disease: a heterogeneous disorder not synonymous with ossification/calcification of the tibial collateral ligament—anatomic and imaging investigation. Skeletal Radiology, 35(12), pp.916-922. PMID: 16988801
- Weaver, M. and Sherman, A. (2020). Pellegrini Stieda Disease. [online] Ncbi.nlm.nih.gov. PMID: 30570968

William Denq, MD CAQ-SM
Department of Emergency Medicine
University of Arizona
@willdenq
Latest posts by William Denq, MD CAQ-SM (see all)
- SplintER Series: Fracture After a Fall From a Bunk Bed - August 6, 2021
- SplintER Series: Open Fracture - May 28, 2021
- SplintER Series: What is Wrong With My Daughter? - May 3, 2021

Gabby Ahlzadeh, MD
Sports Medicine Fellow
University of Utah
Latest posts by Gabby Ahlzadeh, MD (see all)
- SplintER Series: An Easily Missed Shoulder Injury - September 2, 2020
- A Pop in the Calf – Plantaris Rupture - April 15, 2020
- SplintER Series: Delayed pain in an injured knee - March 11, 2020

{kind=link}
{kind=link}
{kind=link}
{kind=link}