

Following intubation the confirmation of endotracheal tube placement and depth is essential. While dynamic etCO2 monitoring has revolutionized the confirmation of endotracheal placement, there are still several circumstances in which this modality may be misleading (e.g. prolonged arrest, severe status asthmaticus/PE/pulmonary edema, etCO2 detector contamination with drugs/gastric contents). Additionally, EtCO2 detectors cannot confirm appropriate endotracheal tube depth, leading to delayed recognition of mainstem placement.
Limitations of current confirmation tools
Chest x-ray, chest ultrasound, and physical exam can be used to confirm appropriate endotracheal tube depth, however, each has limitations. Ultrasound of the chest/pleura can assess for mainstem intubation by evaluating for bilateral pleural sliding. However, it is only about 50% sensitive (i.e. – bilateral lung sliding will occur in 50% of mainstem intubations).1 Chest x-rays are accurate for this purpose, but take significant time from ordering until interpretation. The physical exam for mainstem intubation is notoriously unreliable.2 None of these techniques allow for dynamic assessment of tube placement during repositioning.
Recognizing these issues, we recently developed and validated3 a new ultrasonography technique that we call TRUST (Tracheal Rapid Ultrasound Saline Test) that can provide rapid, accurate assessment of tube placement and facilitate dynamic repositioning.
Trick of the Trade: Tracheal Rapid Ultrasound Saline Test (TRUST)
Our TRUST technique uses point-of-care ultrasonography of the anterior neck to confirm tube placement and position in an average of 4 seconds. The endotracheal tube cuff is inflated with saline rather than air to allow visualization. Cuff visualization at the level of the sternal notch corresponds to an ETT tip that is just inferior to the clavicular heads.
Assessing the endotracheal tube position
- Place a high-frequency linear probe in transverse position over the anterior neck at the level of the sternal notch.

- Deflate the ETT cuff using a 10 mL syringe, noting the volume of air removed.
- Reinflate the cuff using the same volume of normal saline.
- As the saline is being injected attempt to visualize the bright posterior walls of the cuff filling within the trachea. Swirling air bubbles will often be seen.

Ultrasound showing swirling air bubbles from endotracheal tube cuff (transverse view of the anterior neck)
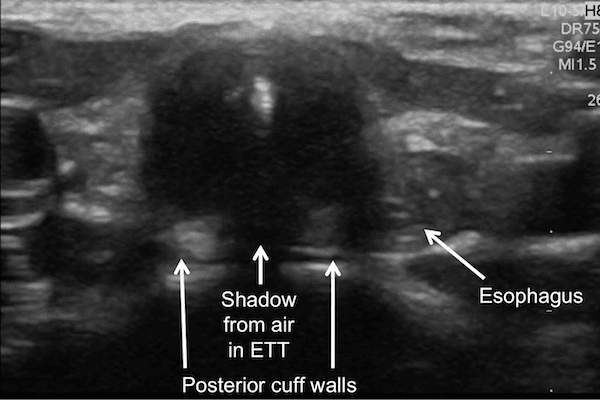
If the cuff is not seen, sweep the probe superiorly along the trachea to the level of the vocal cords to search for the saline-inflated cuff. Once air bubbles have dissolved, the saline inflated cuff is recognized by its posterior wall, appearing as horizontal hyperechoic lines interrupted by shadowing from air within the endotracheal tube.
Repositioning a misplaced tube
The sternal notch is the optimal point for the cuff of the tube.
If the cuff is visualized cephalad to the sternal notch, consider inserting the tube further to prevent extubation. The movement of the cuff can be followed dynamically during repositioning with ultrasound.
What if you cannot see the tube?
If the cuff is not visualized from the sternal notch to the larynx, then the cuff is either deep to the sternum, signifying a tube tip that is likely maintem, or in the esophagus (Read more about recognizing esophageal intubations by ultrasound by Dr. Mark Favot). If there is no evidence of an esophageal intubation, hold the probe at the sternal notch and slowly withdraw the tube until the saline-filled cuff is visualized. As long as your cuff is not overinflated, moving the tube while the cuff is inflated with saline should not cause mucosal damage moving from the smaller mainstem bronchus towards the larger trachea.
If doubt exists whether a saline-filled cuff is being visualized on screen, you can withdraw the saline from the cuff while observing the structure in question. If the structure shrinks and disappears – it was the cuff!

Ultrasound demonstrating deflation of saline-filled cuff of endotracheal tube
Can we TRUST the evidence?
We studied this technique in children undergoing intubation for elective surgeries, and found it took an average of 4 seconds to perform and was 98.8% sensitive and 96.4% specific for correct ETT depth of insertion. However, care should be taken in using this technique with adults, as TRUST has not been validated in patients >18 years of age.
Is it safe to TRUST your tube?
Normal saline is regularly used as a cuff-inflation medium in aeromedical transport and ENT procedures that are associated with a risk of laser-initiated airway fire. There is no evidence that it is associated with any increased risk of cuff rupture. In the unlikely event of a cuff rupture, the volume of saline entering the airway is similar to that used during ETT suctioning and should not pose a risk to the patient. Despite the safety of saline, I usually replace it with air after positioning the tube to limit confusion during handover to other physicians.
Conclusion
TRUST is a novel rapid bedside ultrasound technique that can help optimize endotracheal tube position. It holds great promise in evaluating possible ETT dislodgement in critically ill patients without the delay typically associated with chest radiography, and allows for dynamic tube positioning under real-time sonographic guidance. It is not yet validated in adults – if any readers are interested in collaborating on such a study, please let the author know!
Read more about ultrasonography in the ALiEM Ultrasound for the Win series
References
- 1. Sim S, Lien W, Chou H, et al. Ultrasonographic lung sliding sign in confirming proper endotracheal intubation during emergency intubation. Resuscitation. 2012;83(3):307-312. [PubMed]
- Sitzwohl C, Langheinrich A, Schober A, et al. Endobronchial intubation detected by insertion depth of endotracheal tube, bilateral auscultation, or observation of chest movements: randomised trial. BMJ. 2010;341:c5943. [PubMed]
- Tessaro M, Salant E, Arroyo A, Haines L, Dickman E. Tracheal rapid ultrasound saline test (T.R.U.S.T.) for confirming correct endotracheal tube depth in children. Resuscitation. 2015;89:8-12. [PubMed]

Mark Tessaro, MD
Research Lead, Emergency Point-of-Care Ultrasound Program
Hospital for Sick Children, Toronto
Assistant Professor, University of Toronto


{kind=link}
{kind=link}