

Have you ever been working a shift at 3 am and wondered, “Am I missing something? I’ll just splint and instruct the patient to follow up with their PCP in 1 week.” This is a reasonable approach, especially if you’re concerned there could be a fracture. But we can do better. Enter the “Can’t Miss” series: a series organized by body part that will help identify injuries that ideally should not be missed. This list is not meant to be comprehensive review of each body part, but rather to highlight and improve your sensitivity for these potentially catastrophic injuries. To begin: “Can’t Miss” adult elbow injuries.
The Elbow
- Approximately 5% of all fractures seen in ED involve the elbow.1
- Missed elbow injuries can be highly morbid.
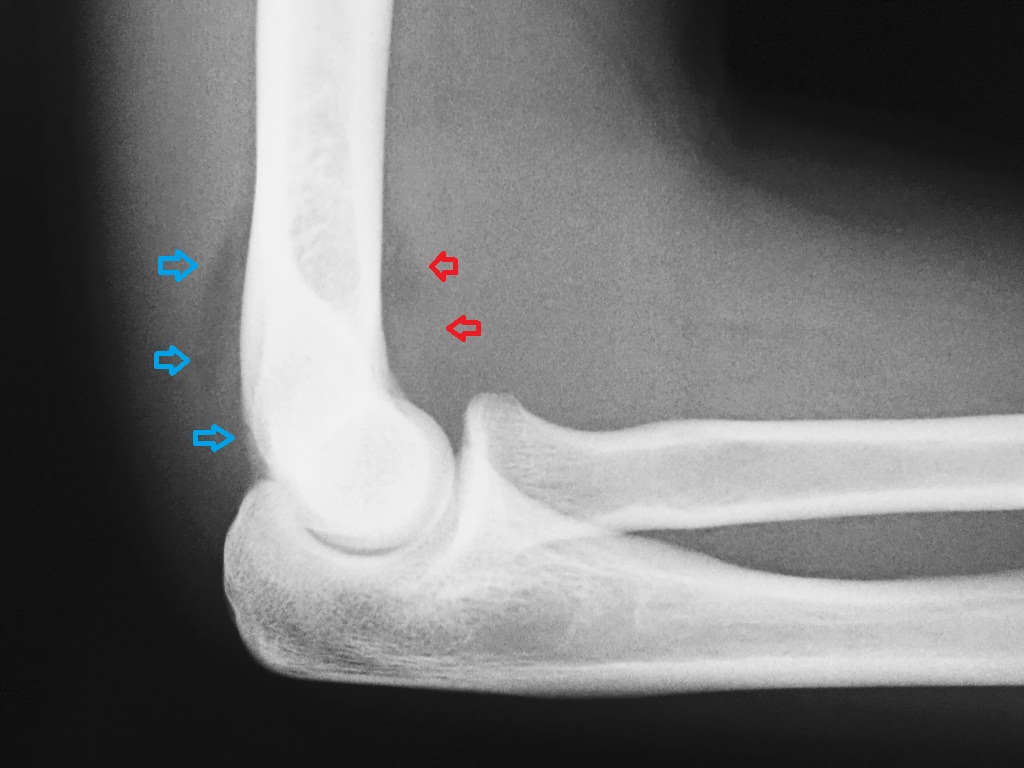
Occult Radial Head Fracture
- Epidemiology: This is the most common elbow fracture in adults.2 They typically occur from a fall onto outstretched hands (FOOSH).
- Symptoms: Patients often complain of pain in lateral elbow.
- Physical Exam: Pain with pronation and supination
- Diagnostic X-ray: Presence of a pathologic fat pad. In adults this is most likely indicative of a radial head or neck fracture.
- Treatment: Sling and rest, ice, compression, elevation (RICE) if non-displaced and 1-week follow-up.3 If displaced or with restricted range of motion, follow-up within 24 hours.2
Coronoid Process Fracture
- Epidemiology: These are uncommon fractures; they are typically associated with posterior elbow dislocation.
- Symptoms: Patients report pain and tenderness to palpation over antecubital fossa. Obvious deformity is likely present if the elbow is dislocated.
- Physical Exam: Tenderness to palpation over antecubital fossa, unstable elbow even after reduction4
- Diagnostic X-ray: These fractures are best seen on lateral view or oblique view. They often require CT for diagnosis.2 If a coronoid fracture is identified on post-reduction films, place a long arm posterior mold splint and arrange follow-up within 24 hours.2

Monteggia Fracture-Dislocation
- Fracture of proximal 1/3 ulna and associated radial head dislocation
- Epidemiology: These fractures typically occur with FOOSH mechanism; they are more common in children.
- Symptoms: Patients report pain and swelling at elbow.
- Physical Exam: Pain, swelling at elbow, limited range of motion
- Diagnostic X-ray: A radial head that does not point toward the capitellum in any views of the elbow suggests a radial head dislocation. If this occurs, obtain forearm and wrist x-rays to assess for an ulnar fracture.
- Treatment: Emergent orthopedic consultation5

Essex-Lopresti Injury
- Fractured radial head, disruption of the distal radio-ulnar joint (DRUJ), and a torn forearm inteosseous membrane (IOM)
- Epidemiology: Thesse fracture typically occur after high impact FOOSH. Rare, but often missed and associated with high morbidity.1
- Symptoms: Patients report pain at elbow.
- Physical Exam: Tender at the elbow and at the wrist
- Diagnostic X-ray: These injuries can occur with any radial head fracture but are typically seen with a comminuted radial head fracture. If a radial head fracture is present, obtain forearm wrist x-rays to assess for DRUJ widening especially if a patient has wrist pain.
- Treatment: These injuries are typically managed operatively.1

Want a more basic approach to traumatic elbow imaging? Check out EMRad’s approach to the traumatic adult elbow.
References
-
1.Goldflam K. Evaluation and treatment of the elbow and forearm injuries in the emergency department. Emerg Med Clin North Am. 2015;33(2):409-421. https://www.ncbi.nlm.nih.gov/pubmed/25892729.
-
2.Bredenkamp J. Injuries to the Elbow and Forearm. In: Tintinalli’s Emergency Medicine. A Comprehensive Guide. 7th ed. New York: McGraw-Hill Education; 2011:1821-1830.
-
3.O’Dwyer H, O’Sullivan P, Fitzgerald D, Lee M, McGrath F, Logan P. The fat pad sign following elbow trauma in adults: its usefulness and reliability in suspecting occult fracture. J Comput Assist Tomogr. 2004;28(4):562-565. https://www.ncbi.nlm.nih.gov/pubmed/15232392.
-
4.Wells J, Ablove R. Coronoid fractures of the elbow. Clin Med Res. 2008;6(1):40-44. https://www.ncbi.nlm.nih.gov/pubmed/18591378.
-
5.Delpont M, Louahem D, Cottalorda J. Monteggia injuries. Orthop Traumatol Surg Res. 2018;104(1S):S113-S120. https://www.ncbi.nlm.nih.gov/pubmed/29174872.

Stephen Villa, MD
Medical Education Fellow
Department of Emergency Medicine
University of California, Los Angeles
Department of Emergency Medicine
University of California, Los Angeles
Latest posts by Stephen Villa, MD (see all)
- EMRad: Radiologic Approach to the Traumatic Hip/Pelvis - September 1, 2021
- EMRad: Can’t Miss Pediatric Elbow Injuries - April 5, 2021
- EMRad: Radiologic Approach to the Pediatric Traumatic Elbow X-ray - March 19, 2021


{kind=link}
{kind=link}
{kind=link}