
The complications of alcohol use can be subtle in older adults, and the effects of alcohol are often incorrectly attributed to aging. Because of its under-recognition, the barriers to screening, and the many subtle ways in which it can present, some have suggested that alcohol misuse has replaced syphilis as the “great masquerader”. If you don’t think alcohol misuse is a problem among older adults in your ED, it may be because it has been hidden in plain sight.
How big is the problem?
Across all age groups, alcohol is a contributing factor in 80,000 deaths and over $223.5 billion in yearly costs to society in the US according to the CDC.1 Among older ED adults, the prevalence of alcohol misuse is around 10-15%.2 Among medical inpatients, 21% of those over 60, and 15% of those over 70 have screened positive for alcohol misuse.3 Among men over age 60 who were drivers in an MVC and admitted to the hospital, 21% had a positive blood alcohol level.4 It has been difficult to quantify the morbidity and mortality attributable to alcohol misuse in older adults, because of the many confounding factors that are introduced with age, poly-pharmacy, and comorbidity.
What qualifies as hazardous alcohol use in an older adult?
The definitions of hazardous or risk drinking vary based on age and gender:1
- For men under 65: more than 14 drinks per week, or more than 4 drinks per occasion
- For women under 65: more than 7 drinks per week, or more than 3 drinks per occasion
- For men and women over 65: more than 7 drinks per week, or more than 3 drinks per occasion
Above these limits, alcohol use is classified as hazardous drinking. However, the safe threshold could be lower for those on certain medications that can put them at risk for adverse medication interactions, particularly sedatives.
What are alcohol abuse and dependence?
The definition of hazardous drinking is based on the number of drinks per week or occasion. Those who drink despite adverse consequences are defined as suffering from alcohol abuse, and those who experience cravings, tolerance, and withdrawal symptoms are categorized as having alcohol dependence.5
We frequently fail to detect alcohol misuse, particularly in older adults
Studies assessing whether alcohol misuse is recognized by physicians caring for older adults show that it is often missed. Despite the high prevalence of alcohol misuse, ED physicians detect only about 20% of older patients with alcohol problems2, and 30-40% are detected among older hospitalized patients.3,6 While it is easy to relegate alcohol screening and treatment to a patient’s primary care physician, many ED patients do not have good access to primary care. Furthermore, in a study of older primary care patients in which 10% screened positive for alcohol misuse, in less than half of the cases had the problem been recognized by the primary care physician.7 This under-recognition likely leads to adverse health outcomes.
Is excessive alcohol use all that dangerous?
There are many chronic diseases that can be caused or exacerbated by excessive alcohol intake. These often manifest later in life after years of alcohol use, so a patient not currently drinking may still suffer damage from prior years of drinking. Some of the diseases associated with chronic alcohol use include:5
- Liver failure and cirrhosis
- Hypertension
- Cognitive impairment/dementia
- Malnutrition and vitamin deficiencies leading to Wernicke-Korsakoff syndrome
- Dysrhythmia
- Cardiomyopathy
- Gastritis
- Depression
- The relationship between alcohol use, depression, and suicide is complex, as patients may drink because of their depression. Alcohol use can make depression more difficult to treat.
- Peripheral neuropathy
- Head and neck cancers
- Prostate and colon cancers
Acute problems associated with alcohol use include many that are every-day occurrences in the ED:5
- Falls or injuries
- It has been difficult to demonstrate a clear causal effect between alcohol and falls because of the many confounding variables). However, falls are highly associated with alcohol use in the general adult population, in whom an alcohol level over 100 mg/dL confers a relative risk of falls of 60.8
- Driving impairment
- Delirium
- Withdrawal
- Adverse drug reactions
- Pancreatitis
- Hypoglycemia
- Alcoholic ketoacidosis
- Suicide – In suicide patients over age 65, 16% had a positive blood alcohol level5
What should we do about it?
1. Think about whether alcohol misuse could be contributing to your patient’s chief complaint.
- Do they have abdominal pain from alcohol-related pancreatitis or gastritis?
- Have they had increasing falls because of alcohol misuse?
- Were they under the influence of alcohol when they had the MVC?
- Do they have malnutrition, or vitamin deficiencies from chronic alcohol use?
- Could their altered mental status be the result of acute alcohol intoxication or withdrawal?
2. Ask your patients about their drinking patterns.
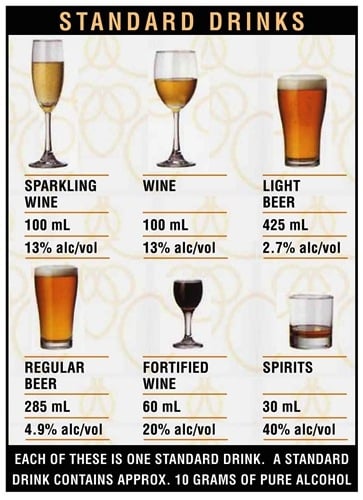
- If you have time to ask only one question, ask whether they drink more than 7 standard drinks on an average week, or if they drink more than three drinks per day. If they answer yes, then you can ask further questions about patterns of drinking and symptoms of dependence and abuse.
3. Consider performing a brief intervention in the ED has been shown to decrease drinking rates among the general adult population.
- The 7 minutes spent on an average brief negotiation interview (BNI) may feel like a long time in a busy ED, but the effects are profound.9 The BNI is a scripted means of discussing dangerous behaviors such as alcohol or substance abuse with the patient in a non-confrontational way, helping to develop a plan with which the patient agrees and specific goals for their drinking habits (see here for the basic steps1). Performing a BNI has been found by many studies to decrease levels of alcohol consumption even up to a year later.10
- Other studies of brief interventions in a range of clinical settings have shown reduction in future injuries and DUIs.11,12 Cost-benefit analysis of brief interventions among admitted patients for reduction of future health care costs have shown a benefit of about $4 for each $1 spent on screening and intervention.13 If you have the resources available, you can also refer the patient for alcohol counseling or to their primary physician for follow up. Screening and brief intervention for alcohol abuse is also recommended by ACEP.
“The ACEP believes alcohol abuse is a significant public health problem. Furthermore, ACEP believes emergency medical professionals are positioned and qualified to mitigate the consequences of alcohol abuse through screening programs, brief intervention, and referral to treatment. ACEP encourages wide availability of resources necessary to address the needs of patients with alcohol-related problems and those at risk for them.”
The Bottom Line
Alcohol misuse is prevalent among older adults. It can cause serious acute and chronic health problems. We are failing to identify alcohol misuse in the ED in patients of all ages, but particularly in older patients. If identified, we can potentially intervene with counseling or referral for treatment. If you don’t think about it, you may miss it.

Department of Emergency Medicine
University of North Carolina - Chapel Hill
@clshenvi
Latest posts by Christina Shenvi, MD, PhD, MBA (see all)
- The Most Dangerous 10 Minutes of Your Shift: Mastering the ED Hand-Off - October 30, 2025
- The First Pulse Check: How to set yourself up for success in EM residency - April 9, 2025
- How I Educate Series: Christina Shenvi, MD - January 4, 2023



{kind=link}
{kind=link}
{kind=link}