

This is EMRad, a series aimed at providing “just in time” approaches to commonly ordered radiology studies in the emergency department. When applicable, it will provide pertinent measurements specific to management, and offer a framework for when to get an additional view, if appropriate. Last post, we focused on the elbow. Now: the wrist.
Learning Objectives
- Interpret traumatic wrist x-rays using a standard approach.
- Identify clinical scenarios in which an additional view might improve pathology diagnosis
Why the wrist matters and the radiology rule of 2’s
The Wrist
- 25% of all sports-related injuries involve the hand or wrist.1
- Approximately 1.5% of all ED visits involve the hand and forearm.2
- Missed wrist injuries can be highly morbid.
- Missed wrist injuries are a common area of litigation.
Before we begin: Make sure to employ the rule of 2’s3
- 2 views: One view is never enough.
- 2 abnormalities: If you see one abnormality, look for another.
- 2 joints: Image above and below (especially for forearm and leg).
- 2 sides: If unsure regarding a potential pathologic finding, compared to another side.
- 2 occasions: Always compare with old x-rays if available.
- 2 visits: Bring the patient back for repeat films.
An approach to the traumatic wrist x-ray
- Adequacy/Alignment
- Bones
- Distal radius
- Distal ulna
- Carpal bones
- Carpal/metacarpal alignment
- Perilunate/lunate dislocation
- Gilula’s Lines
- Carpometacarpal dislocation
- Distal radioulnar joint (DRUJ) subluxation/dislocation
- Consider an additional view
1. Adequacy
- PA View
- Check for rotation. There should be no overlap of radius and ulna.
- The view should include distal radius and ulna.

- Lateral View
- Check for rotation. There should be a perfect overlap of radius and ulna.
- Identify the distal radius, lunate and capitate. They should make a straight line.
2. Bones
- Distal radius and ulnar styloid
- On the AP view, the distal radius should cup the carpals and the most distal portion of the articular surface should be radial styloid (radiocarpal joint).
- On the lateral view, the radial surface should be smooth. If it is not, consider possible distal radius fracture.
- Trace the ulnar styloid: If it is not, interrogate the ulna for a possible fracture.
- Pearl: This injury is usually not isolated, so look carefully for a second fracture.


- Carpal Bones
- Trace cortex of all carpal bones.
- Look specifically at the scaphoid. If there is a high suspicion for injury, consider scaphoid view/series.

3. Carpal/Metacarpal and Joint Alignment
- Lateral view:
- Draw a line through distal radius, lunate and capitate. If they do not make a straight line, think distal radius fracture, perilunate, or lunate dislocation.
- The lunate should sit within cup of radius and capitate should be directly above lunate. If it does not, consider perilunate or lunate dislocation.
- AP view
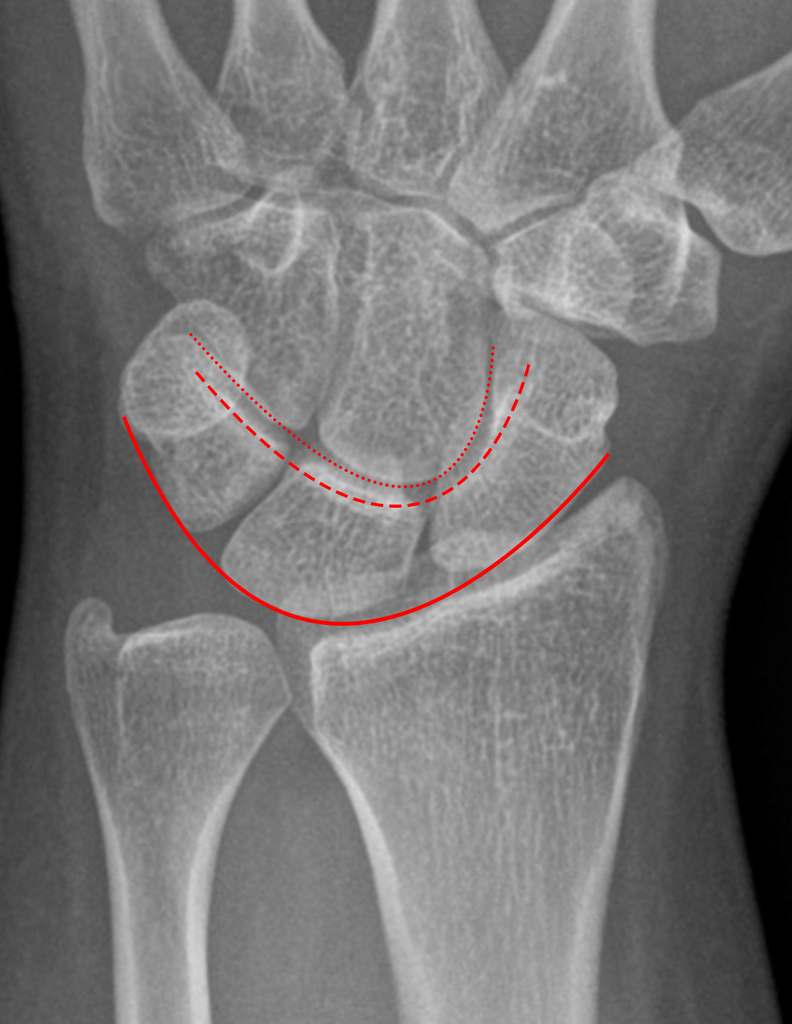
- Carpal bones are arranged in 2 rows forming 3 smooth arcs (Gilula’s arcs) and separated by 1-2 mm space. If there is a break in the arc, think carpal bone fracture or ligamentous injury.
- Look specifically at scaphoid and lunate for widening. If widening is present, think scapholunate dissociation and consider obtaining a “clenched fist” view.
On AP and Lateral, the joint space between distal row and carpals should be visible. If it is not, think carpometacarpal dislocation. Sometimes, this dislocation is easiest to see on lateral (see Figure 7).



- On AP, if there is > 2 mm widening between the distal radius and ulna, think distal radioulnar joint subluxation/dislocation and check lateral.4 The dislocation should be evident on lateral films.


4. Consider an Additional View
Scaphoid view or series
- When: High suspicion for scaphoid fracture
- Why: Obtaining the film with the patient in ulnar deviation should make the scaphoid easier to see.

The “clenched fist” view
- When: High suspicion for scapholunate dissociation
- Why: Clenching the fist will widen the space between scaphoid and lunate, which suggests a scapholunate dissociation.

“Carpal tunnel” view
- When: Consider this view when a patient has pain at hypothenar eminence or a sensory deficit in the ulnar distribution.
- Why: If fractured, the hook of hamate can displace into Guyon’s Canal causing ulnar nerve sensory changes.

Read more about positive findings in our SplintER Series: Common ED Splint Techniques.
Afraid you might miss something commonly missed or catastrophic? Can’t Miss wrist injuries.
Want a more in-depth approach to wrist radiography? Check out radiopaedia’s approach to the wrist.
References:
-
1.Avery, D et al. Sports-related wrist and hand injuries: a review. Journal of Orthopaedic Surgery and Research, Vol 11, No 99, September 2016. https://www.ncbi.nlm.nih.gov/pubmed/27633260.
-
2.Chung KC, SSV. The frequency and epidemiology of hand and forearm fractures in the United States. The Journal of Hand Surgery Am, Vol 26, No 5, September 2001. https://www.ncbi.nlm.nih.gov/pubmed/11561245.
-
3.Chan, OttoI. ABCs and Rules of Two. ABC of Emergency Radiology. Third Edition.Edited by Otto Chan. 2013 John wiley & Sons, Ltd. Published 2013. .
-
4.Nakamura R, Horii E, IT Tsunoda K, Nakao E. Distal radioulnar joint subluxation and dislocation diagnosed by standard roentgenography. Skeletal Radiol, Vol 24, No 2, February 1995. https://www.ncbi.nlm.nih.gov/pubmed/7747190.

Stephen Villa, MD
Department of Emergency Medicine
University of California, Los Angeles
Latest posts by Stephen Villa, MD (see all)
- EMRad: Radiologic Approach to the Traumatic Hip/Pelvis - September 1, 2021
- EMRad: Can’t Miss Pediatric Elbow Injuries - April 5, 2021
- EMRad: Radiologic Approach to the Pediatric Traumatic Elbow X-ray - March 19, 2021


{kind=link}
{kind=link}
{kind=link}