

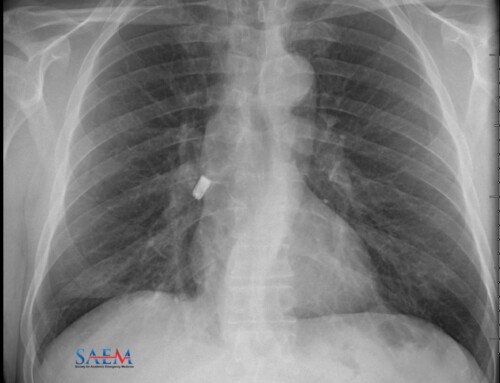
A 51-year-old female with a history of metastatic ovarian cancer on chemotherapy, malignant pleural effusions requiring repeat thoracentesis, and pulmonary embolism presented to the Emergency Department with worsening shortness of breath and dry cough. Upon arrival, she was hypoxic with an oxygen saturation level of 75% on room air. She was tachycardic, tachypneic, and her blood pressure was 125/56 mmHg. Labs revealed only a mild anemia (Hgb: 10.2). It was determined that her symptoms were secondary to recurrent right-sided malignant pleural effusions. Her presenting chest X-ray is pictured above (Image 1: Author’s own image).
Because of the patient’s debilitating symptomatology, a right-sided bedside thoracentesis was performed. 1.5 L of thin, dark brown fluid was removed and after the procedure, the patient stated she felt much better. Repeat vital signs after thoracentesis revealed: HR 105 bpm, RR 18 rpm, O2 saturation of 98% on room air. Blood pressure remained stable. A repeat chest x-ray was performed:

Image 2: Patient’s x-ray after thoracentesis (author’s own image).
Trapped lung syndrome. This syndrome occurs when fluid is drained from the pleural cavity, but the lung fails to expand due to improper pleural healing after inflammation [1, 2]. This is typically caused by a chronic inflammatory process such as recurrent pleural effusions. Approximately 32% of patients receiving recurrent thoracenteses may ultimately develop trapped lung syndrome; identification should be a point of emphasis in patients undergoing thoracentesis [3]. Trapped lung syndrome can also be caused by coronary artery bypass graft, uremia, thoracic radiation, pericardiotomy, bacterial pleuritis, and parapneumonic pleural effusions [4]. Lung entrapment has been commonly used interchangeably with the term trapped lung, but these similar terms have subtle differences as entrapment refers to active inflammatory pleuritis or other non-pleural causes while trapped lung is secondary to chronic fibrosis and collagen deposition [2].
It is vital to differentiate a pneumothorax from trapped lung syndrome; these conditions may look similar on chest X-rays, but their management differs significantly. Some key differentiating features:
- In a typical pneumothorax, air should rise to the apical region when viewed on upright chest x-ray.
- On CT, pleural fibrosis and thickness is more consistent with trapped lung.
Identifying the correct diagnosis changes the management plan and avoids unnecessary procedures. For instance, the placement of a chest tube results in reinflation of the lung in the setting of a pneumothorax, but this procedure would not provide any resolution in the setting of a trapped lung, as evidenced by this patient’s post-chest tube x-ray.

Image 3: Patient’s x-ray after placement of a pigtail catheter (author’s own image).
Many patients with trapped lung syndrome will develop recurrent pleural effusions. However, despite the presence of pleural effusion and trapped lung, many patients remain asymptomatic. Asymptomatic patients do not require any treatment for trapped lung or for their pleural effusion. If the patient is symptomatic, as this patient was, thoracentesis may offer temporary relief because removing pleural fluid will allow for better movement of the diaphragm. Thoracentesis will not alleviate the trapped lung, however. In some cases, patients may require decortication of the visceral pleura, which may allow for re-expansion of the trapped lung and a decreased recurrence of pleural effusions [5].
Because the patient was on therapeutic anticoagulation and imaging was highly suspicious for trapped lung, chest tube placement in the ED was deferred and the patient was admitted to the hospital for observation. She later received a right-sided chest tube which was performed by interventional radiology, as her symptoms began to worsen while she was in the hospital. The chest tube did not significantly alleviate her symptoms nor did it inflate the trapped lung. The patient was eventually discharged home with hospice care.
References
Want more visual diagnosis? We see you! Check out ALiEM’s archives for Diagnose on Sight, SAEM’s Clinical Images, and ACMT’s Visual Pearls.
- Doelken P, Sahn SA. Trapped lung. Semin Respir Crit Care Med. 2001;22(6):631-636. PMID: 16088707
- Huggins JT, Doelken P, Sahn SA. The unexpandable lung. F1000 Med Rep. 2010;2:77. PMID: 21173837
- Divietro M, Huggins J, Doelken P, Gurung P, Kaiser L, Sahn S. Prevalence and causes of unexpandable lung over a ten-year period. Chest. 2011;140:700A.
- Huggins JT, Sahn SA, Heidecker J, Ravenel JG, Doelken P. Characteristics of trapped lung: pleural fluid analysis, manometry, and air-contrast chest CT. Chest. 2007;131(1):206-213. PMID: 17218577
- Doelken P. Clinical implications of unexpandable lung due to pleural disease. Am J Med Sci 2008; 335:21 PMID: 18195579
- Khan H, Fernandez-Perez E R, Caples S M. Post-thoracentesis trapped lung. J Postgrad Med 2007;53:119-20. PMID: 17495380
- Cantey EP, Walter JM, Corbridge T, Barsuk JH. Complications of thoracentesis: incidence, risk factors, and strategies for prevention. Curr Opin Pulm Med. 2016;22(4):378-385. PMID: 27093476

Prabdit Sidhu
California Northstate University
Latest posts by Prabdit Sidhu (see all)
- Is it a Pneumothorax? An Unusual Post-Thoracentesis Radiograph - September 30, 2020

Nathan Stuempfig, DO, FACEP
Assistant Clinical Professor, Emergency Medicine
Benard J. Tyson, Kaiser Permanente School of Medicine
Latest posts by Nathan Stuempfig, DO, FACEP (see all)
- Is it a Pneumothorax? An Unusual Post-Thoracentesis Radiograph - September 30, 2020


{kind=link}
{kind=link}
{kind=link}