
Welcome to another ultrasound-based case, part of the “Ultrasound For The Win!” (#US4TW) Case Series, where bedside ultrasound changed the management or aided in a diagnosis. In this case, an 18-year-old man presents with acute shoulder pain after an injury.
Learning Objectives
- List the differential diagnosis for a patient presenting with shoulder pain.
- Discuss the role of the shoulder point-of-care ultrasound (POCUS) and how to correctly perform the scan using a posterior approach.
- Discuss the prevalence, diagnostic approach, sonographic findings, ED management, and disposition of a shoulder subluxation.
- Discuss recent literature regarding shoulder POCUS and its utility and value in the ED, particularly in shoulder dislocations.
Case Presentation
An 18-year-old male with no past medical history presents to the ED with acute-onset left shoulder pain that occurred just prior to arrival. The patient was involved in a physical altercation in which his left arm was pulled. He felt a “pop” followed by pain in the shoulder. The patient reports that his arm was pulled again a second time, further worsening the pain. He complains of persistent limited and painful range of motion (ROM) of the left shoulder. He has no history of prior shoulder dislocations, fractures, or other musculoskeletal injuries.
On physical examination, the patient’s left shoulder has limited active ROM due to pain but is able to perform abduction of more than 90 degrees, and internal and external rotation of the affected joint. There is tenderness to palpation of the anterolateral aspect of the left shoulder but no redness, significant swelling, or any obvious deformities.
Vitals
- BP 110/65 mmHg
- HR 85 bpm
- RR 20 breaths/min
- SpO2 95% on room air
- Temp 36.4⁰C
Differential Diagnosis
- Shoulder dislocation
- Glenohumeral joint (GHJ) effusion
- Shoulder subluxation / GHJ instability
- Acromioclavicular (AC) joint injury
- Shoulder sprain/strain
- Proximal humerus fracture
- Clavicle fracture
- Scapular fracture
- Rotator cuff tear
- Biceps or triceps tendon injuries
Our Clinical Approach
Upon physical examination, there was a low clinical suspicion for shoulder dislocation, given the patient’s decent ROM. The clinical presentation suggested a shoulder sprain versus a partial tear of the rotator cuff muscles versus GHJ instability or subluxation, which may be secondary to above.
While an x-ray would be the usual initial imaging modality of choice in a patient presenting to the ED with a musculoskeletal injury, there can be delays in obtaining imaging depending on patient volumes, staffing, and resources. Given this, a bedside POCUS of the shoulder was performed using a posterior approach in order to quickly rule out a shoulder dislocation and expedite patient care.



Diagnosis: Shoulder Subluxation
- Also known as shoulder or glenohumeral joint partial dislocation, or glenohumeral joint instability.
- Occurs when the humeral head partially slides (or “dislocates”) in and out of place with range of motion at the GHJ. It is usually associated with trauma to the shoulder and injury to the shoulder ligaments. It can also occur in the absence of trauma, in which case it is typically associated with congenital instability of the GHJ.
- The role of the ED physician involves ruling out a shoulder dislocation, concomitant fractures, or neurovascular injuries. Usually, no reduction attempt is required (unless the diagnosis is not certain and there is concern for an actual dislocation), and the patient can be discharged home with a shoulder sling or immobilizer as well as a plan for analgesia, such as anti-inflammatories.
- Any patient with shoulder subluxation should be referred to outpatient orthopedic follow up as they will likely need further imaging and evaluation for both non-operative and surgical options for definitive treatment.

Shoulder POCUS: The Posterior Approach
- Position yourself behind the patient with the ultrasound machine positioned in front of the patient.
- Locate the scapular spine with palpation.
- Using the curvilinear probe, place the probe on top of the scapular spine in a transverse plane with the probe orientation marker pointing toward to the patient’s left (Fig. 4). Identify the scapular spine as a hyperechoic line with posterior shadowing. Note the deltoid and the infraspinatus muscle above the scapular spine.
- Slide the probe laterally along the scapular spine, towards the GHJ. You will start to see the glenoid fossa (which may be difficult to visualize in a non-dislocated shoulder) followed by the humeral head, seen as a round hyperechoic structure with posterior shadowing (Fig. 5).
- To optimize your image, you should position the glenoid fossa and GHJ in the center of the screen. You will see the scapular spine on one half of the screen and the humeral head on the other half. We recommend you adjust the depth for optimal visualization of the GHJ.
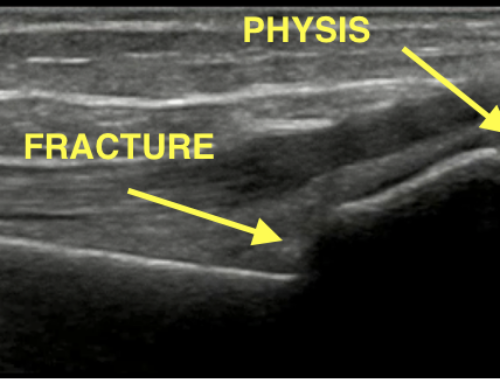
- Remember that if you are scanning the patient’s left shoulder (as in the featured case – Figs. 1, 2), you will see the humeral head on the left side of the screen and the scapular spine on the right side, and vice versa if you are scanning the right shoulder (Figs. 4, 5).
- With a posterior approach, an anterior dislocation is identified as the humeral head is displaced inferiorly on the screen (i.e. away from the probe) (Fig. 6). A posterior dislocation is identified as the humeral head is displaced towards to the top of the screen (i.e. towards the probe).



Shoulder POCUS Tips
- Have the patient slowly rotate the shoulder internally and externally to more easily identify the humeral head (Fig. 7). This will be especially useful to aid in identifying structures in patients with more musculature and/or a larger body habitus.
- If you have any doubt and/or you’re not convinced that the findings are normal or not, scan the unaffected shoulder and compare both sides.
- With the same posterior approach mentioned above, you can perform an ultrasound-guided GHJ lidocaine injection. Remember this procedure should be sterile! Prep the skin with chlorhexidine, use sterile gloves, sterile gel, and probe cover. You will likely need a spinal needle to reach the GHJ. Inject 15-20 cc of 1% lidocaine into the GHJ. Performing intra-articular anesthesia has been described as an effective pre-reduction approach for analgesia with no significant difference in successful reduction rates or pain during or post-reduction; fewer adverse effects; and decrease overall ED length of stay [1].
- In the case of shoulder dislocations, obtain a post reduction x-ray (particularly if the pre-reduction x-ray was not performed) to evaluate for concomitant fractures and to confirm reduction. However, re-scanning the shoulder immediately post-reduction will not only confirm reduction in real time, but also minimize time delays if the shoulder was not successfully reduced and will need a re-attempt of the reduction. This approach will be of more value when doing procedural sedation, as you can potentially re-attempt the reduction while the patient is still sedated. Procedural sedation in a busy ED is a very time and resource-consuming procedure and doing a post-reduction POCUS is a great way to maximize efficiency in utilization of ED resources.
Shoulder POCUS Literature Review
POCUS is a quick and highly accurate way to diagnose shoulder dislocations and subluxations while minimizing length of stay in the ED.
- Secko et al [2] – Study of 65 patients that demonstrated a sensitivity and specificity of 100% (95% CI 87-100%) and 100% (95% CI 87-100%), respectively, for the diagnosis of shoulder dislocations. The “time from triage to diagnosis via POCUS” was a stunning 19 seconds in comparison to 43 minutes of “time from triage to diagnosis via X-ray”. Of note, the images in this study were obtained by ultrasound fellowship trained physicians only.
- Gottlieb et al [3] – Meta-analysis of 306 dislocations. POCUS was 99.1% sensitive (95% CI 84.9-100%) and 99.9% specific (95% CI 88.9-100%) for the diagnosis.
The sooner you attempt reduction, the better your chances at success!
- Kanji et al [4] – Time from “injury to 1st reduction attempt” and “ED arrival to 1st reduction attempt” – both were found to be independent predictors of a higher reduction failure rate (OR=1.07, 95% CI 1.02-1.13; OR=1.19, 95% CI 1.05-1.34). Every interval of 10 minutes increased the odds of a failed reduction attempt by 7% and 19%, respectively, for each group.
Disposition and Case Conclusion: Glenohumeral Subluxation
The patient was placed in a shoulder sling and discharged home with instructions to take ibuprofen as needed for pain. He was instructed to rest the shoulder for the next few days and follow up with his primary care physician with consideration of physical therapy for shoulder strengthening exercises. Lastly, he was referred for outpatient orthopedic followup, as he may need further imaging (i.e. shoulder CT scan or MRI) and potential surgical intervention, if the symptoms persist.
Take Home Points
- Shoulder POCUS is a valuable tool that forms part of the ED physician armamentarium to tackle the diagnosis, ED management, and timely disposition of shoulder injuries.
- Shoulder subluxation is a musculoskeletal injury that can be reliably assessed with POCUS. The ED management consists of ruling out fractures and dislocations, pain management, shoulder movement restriction with shoulder slings or immobilizers, patient education, and adequate outpatient referral to orthopedics or physical therapy.
- Recently published literature illustrated the benefits and effectiveness of shoulder POCUS to reliably diagnose shoulder dislocations, assist in GHJ intra-articular joint injections, and confirm reductions in real time.
Edited by Dr. Jeffrey Shih, Ultrasound For The Win (US4TW) Series Editor
References
- Wakai A, O’Sullivan R, McCabe A. Intra-articular lignocaine versus intravenous analgesia with or without sedation for manual reduction of acute anterior shoulder dislocation in adults. Cochrane Database Syst Rev. 2011;(4):CD004919. Published 2011 Apr 13. doi:10.1002/14651858.CD004919.pub2. PMID: 21491392
- Secko MA, Reardon L, Gottlieb M, et al. Musculoskeletal Ultrasonography to Diagnose Dislocated Shoulders: A Prospective Cohort. Ann Emerg Med. 2020;76(2):119-128. doi:10.1016/j.annemergmed.2020.01.008. PMID: 32111508
- Gottlieb M, Holladay D, Peksa GD. Point-of-care ultrasound for the diagnosis of shoulder dislocation: A systematic review and meta-analysis. Am J Emerg Med. 2019;37(4):757-761. doi:10.1016/j.ajem.2019.02.024. PMID: 30797607
- Kanji A, Atkinson P, Fraser J, Lewis D, Benjamin S. Delays to initial reduction attempt are associated with higher failure rates in anterior shoulder dislocation: a retrospective analysis of factors affecting reduction failure. Emerg Med J. 2016;33(2):130-133. doi:10.1136/emermed-2015-204746. PMID: 26113487

Mark Rivera-Morales, MD
Department of Emergency Medicine
UCF HCA GME Consortium EM Residency
Osceola Regional Medical Center
Latest posts by Mark Rivera-Morales, MD (see all)
- SAEM Clinical Images Series: Breast Swelling - August 29, 2022
- Ultrasound for the Win! 18M with Acute Shoulder Injury #US4TW - November 11, 2020

Fernando Rivera, MD
University of Central Florida College of Medicine
UCF/HCA Emergency Medicine Residency Program of Greater Orlando
Osceola Regional Medical Center
Latest posts by Fernando Rivera, MD (see all)
- Ultrasound for the Win! 18M with Acute Shoulder Injury #US4TW - November 11, 2020

Nicholas Fusco, DO
Emergency Medicine Faculty
University of Central Florida College of Medicine
UCF/HCA Emergency Medicine Residency Program of Greater Orlando
Osceola Regional Medical Center
Latest posts by Nicholas Fusco, DO (see all)
- Ultrasound for the Win! 18M with Acute Shoulder Injury #US4TW - November 11, 2020

Javier Rosario, MD FACEP
Emergency Ultrasound Fellowship Director
Assistant Professor of Emergency Medicine
University of Central Florida College of Medicine
UCF/HCA Emergency Medicine Residency Program of Greater Orlando
Osceola Regional Medical Center
Latest posts by Javier Rosario, MD FACEP (see all)
- Ultrasound for the Win! 18M with Acute Shoulder Injury #US4TW - November 11, 2020

{kind=link}
{kind=link}
{kind=link}