SAEM Clinical Images Series: Male Weightlifter with Chest Pain

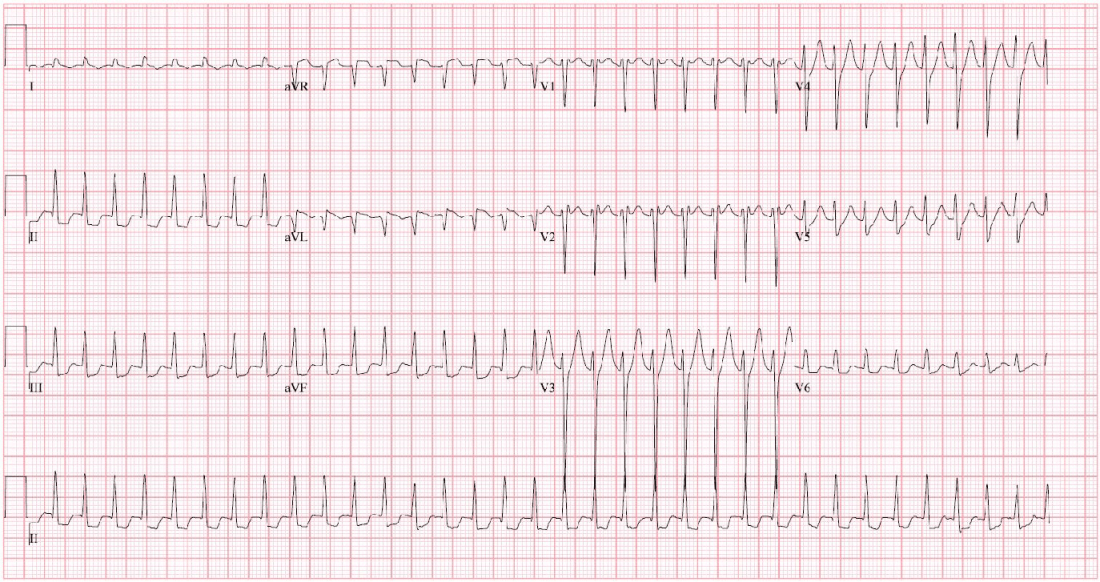
An otherwise healthy 45-year-old male presented to the emergency department (ED) with substernal chest pain radiating down his left arm over the previous two days. On the first day of symptoms, his pain began several hours after using a new pre-workout supplement and weightlifting. The symptoms lasted for a few hours and self-resolved. The pain returned the following day under the same conditions, although this time persistent, which brought him in for evaluation. Associated symptoms included shortness of breath, nausea, and one episode of emesis. He denied pleuritic pain, lower extremity edema, hemoptysis, syncope, cough, or chest wall trauma. On further history, he reported prior use of anabolic steroids, with the last being six weeks prior to presentation. It was unclear what were the contents of the pre-workout supplement, but he denied any tobacco or illicit drug use. Notably, he had a significant family history of heart disease with his father having undergone coronary bypass at age 47. His initial ECG (Image 1) and interval ECG (Image 2) are shown.

Vitals: T 36.5°C; HR 74; RR 16; BP 161/107; SpO2 98% on RA
General: Uncomfortable and diaphoretic in moderate distress.
Cardiovascular: Normal rate and rhythm, no murmurs. Equal radial and PT pulses bilaterally.
Pulmonary: Non-labored breathing, lungs CTA bilaterally with equal breath sounds.
Extremities: Lower extremities without significant edema, symmetric in size.
Neuro: Alert and oriented, neurologically intact.
Complete blood count (CBC): mild polycythemia (Hgb 19.0 g/dL) and leukocytosis (WBC 10.1 x 10(9)/L)
Basic metabolic panel (BMP): Cr 1.22 mg/dL, GFR 75 mL/min/BSA, K 4.5 mmol/L
Troponin T, 5th generation: 97 ng/L (ref. range: <=15 mg/L)
Acute coronary syndrome (ACS) with myocardial infarction. Hyperacute T waves are seen on the initial ECG.
This patient’s initial ECG (Image 1) raised concern for hyperacute T waves, which are often described as broad-based with a large amplitude. This subtle finding is difficult to differentiate from normal variants, hypertrophy, or hyperkalemia (1,2). Hyperacute T waves have been considered an early sign of acute coronary occlusion, however, current literature is mixed regarding their clinical utility, particularly given the lack of a formal ECG definition (3,4,5). The American College of Cardiology (ACC) recommends obtaining serial ECGs in patients with hyperacute T waves to assess for progression to STEMI (3). In this patient’s case, interventional cardiology was consulted, and the patient was given aspirin and sublingual nitroglycerin. He developed worsened chest pain, and a repeat ECG showed no significant changes. Shortly after, he went into ventricular fibrillation and cardiac arrest. A post-ROSC ECG (Image 2) showed concave ST elevations in the anterolateral leads with reciprocal ST depressions in the inferior leads, meeting STEMI criteria. Coronary angiography showed severe multivessel disease and 100% occlusion of the left anterior descending (LAD) artery. A drug-eluting stent was placed, and the patient was discharged home one week later with an intact neurologic status.
History of anabolic steroid use, pre-workout supplementation, and significant family history of CAD. In more recent years, the number of younger patients (35-54 years) hospitalized for ACS has increased (6). This trend is believed to be related to the increased use of illicit drugs, including marijuana and androgenic-anabolic steroids (AAS) (6). AAS is known to increase the risk of cardiac hypertrophy, ACS, and sudden cardiac death by increasing lipoprotein production, causing intimal hyperplasia of coronary arteries, and increasing clotting factors leading to a procoagulant state (7,8). Consensus on the adverse effects and overall safety of pre-workout supplements remains under debate and they remain unregulated by the FDA. Studies suggest that synephrine, a common product found in pre-workout supplements, may raise safety concerns due to its androgenic properties (9). A 2023 systematic review of adverse outcomes related to synephrine found associations with cardiomyopathy, ACS, arrhythmias, and cerebrovascular disease (9,10).
Take-Home Points
-
Hyperacute T waves, although not diagnostic in isolation, may be an early marker for occlusion myocardial infarction and if seen, serial ECGs should be performed.
-
A high degree of clinical suspicion for ACS should be maintained among patients with a history of androgenic-anabolic steroid use, even in young and otherwise healthy individuals.
-
Pre-workout supplements, especially those that contain the compound synephrine have been associated with ACS and other cardiovascular pathology.
-
Somers MP, Brady WJ, Perron AD, et al. The prominent T wave: electrocardiographic differential diagnosis. Am J Emerg Med 2002 May;20(3):243-51
-
Levis JT. ECG Diagnosis: Hyperacute T Waves. Perm J. 2015 Summer;19(3):79. doi: 10.7812/TPP/14-243. PMID:26176573; PMCID: PMC4500486.
-
Writing Committee; Kontos MC, de Lemos JA, Deitelzweig SB, Diercks DB, Gore MO, Hess EP, McCarthy CP, McCord JK, Musey PI Jr, Villines TC, Wright LJ. 2022 ACC Expert Consensus Decision Pathway on the Evaluation and Disposition of Acute Chest Pain in the Emergency Department: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2022 Nov 15;80(20):1925-1960. doi: 10.1016/j.jacc.2022.08.750. Epub 2022 Oct 11. PMID: 36241466; PMCID: PMC10691881.
-
Koechlin L, Strebel I, Zimmermann T, Nestelberger T, Walter J, Lopez-Ayala P, Boeddinghaus J, Shrestha S, Arslani K, Stefanelli S, Reuthebuch B, Wussler D, Ratmann PD, Christ M, Badertscher P, Wildi K, Giménez MR, Gualandro DM, Miró Ò, Fuenzalida C, Martin-Sanchez FJ, Kawecki D, Bürgler F, Keller DI, Abächerli R, Reuthebuch O, Eckstein FS, Twerenbold R, Reichlin T, Mueller C; APACE investigators. Hyperacute T Wave in the Early Diagnosis of Acute Myocardial Infarction. Ann Emerg Med. 2023 Aug;82(2):194-202. doi: 10.1016/j.annemergmed.2022.12.003. Epub 2023 Feb 10. PMID: 36774205.
-
Smith SW, Meyers HP. Hyperacute T-waves Can Be a Useful Sign of Occlusion Myocardial Infarction if Appropriately Defined. Ann Emerg Med. 2023 Aug;82(2):203-206. doi: 10.1016/j.annemergmed.2023.01.011. Epub 2023 Mar 3. PMID: 36872197.
-
Bhatt DL, Lopes RD, Harrington RA. Diagnosis and Treatment of Acute Coronary Syndromes: A Review. JAMA. 2022;327(7):662-675.
-
Melchert RB, Welder AA. Cardiovascular effects of androgenic-anabolic steroids. Med Sci Sports Exerc. 1995;27(9):1252-1262.
-
Pope HG, Jr., Kanayama G, Athey A, Ryan E, Hudson JI, Baggish A. The lifetime prevalence of anabolic-androgenic steroid use and dependence in Americans: current best estimates. Am J Addict. 2014;23(4):371-377.
-
de Jonge MLL, Kieviet LC, Sierts M, Egberink LB, van der Heyden MAG. Review of Case Reports on Adverse Events Related to Pre-workout Supplements Containing Synephrine. Cardiovasc Toxicol. 2023 Jan;23(1):1-9. doi: 10.1007/s12012-022-09777-z. Epub 2023 Jan 13. PMID: 36639595; PMCID: PMC9859859.
-
Flo FJ, Kanu O, Teleb M, Chen Y, Siddiqui T. Anabolic androgenic steroid-induced acute myocardial infarction with multiorgan failure. Proc (Bayl Univ Med Cent). 2018;31(3):334-336