

Have you ever been working at 3am and wondered, “Am I missing something? I’ll just splint and instruct the patient to follow up with their PCP in 1 week.” This is a reasonable approach, especially if you’re concerned there could be a fracture. But we can do better. Enter the “Can’t Miss” series: a series organized by body part that will help identify injuries that ideally should not be missed. This list is not meant to be a comprehensive review of each body part, but rather to highlight and improve your sensitivity for these potentially catastrophic injuries. We’ve already covered the elbow and wrist. Now: the foot and ankle.
The Ankle/Foot
- 4% of all visits to the ED involve the ankle [1].
- The foot is a complex part of human anatomy and is a frequent cause for a visit to the Emergency Department [2].
- High morbidity if unstable injuries are missed.
Epidemiology/Importance: One of the most common tendon injuries of adults. Typically occurs after sudden plantarflexion or forced dorsiflexion of foot.
Symptoms: Sudden “pop” or as though they got “hit” in the back of the ankle. May have difficulty walking.
Physical Exam: Tenderness can be noted from calf down to the heel. There may be a palpable defect at the achilles. Make sure to check the Thompson Test. Note, this test may be falsely negative if a partial tear exists.
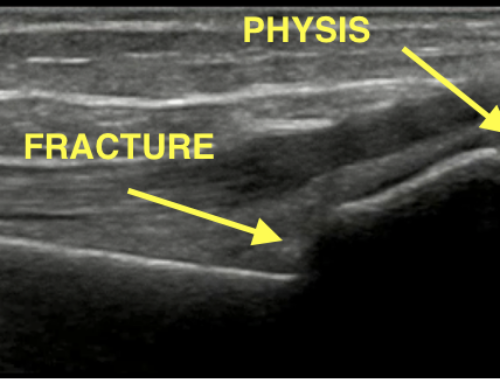
Diagnostic Imaging: Although not always present, look for pre-achilles fat pad (Kager’s fat pad) distortion on plain film (figure 1). Consider ultrasound to assess for partial versus full thickness tear.
Treatment: Non weight-bearing, Posterior splint in Equinus Position (20 degrees plantarflexion).
Check out CoreEM’s post on Achilles tendon rupture for more information.

Figure 1: Achilles tendon rupture with associated Kager’s Fat pad highlighted in red. Case courtesy of Dr Pir Abdul Ahad Aziz, Radiopaedia.org
Epidemiology/Importance: Suspect this injury with mechanisms including dorsiflexion and external rotation (eg. football, basketball, rugby, hockey, skiing, etc.) [3]. This injury is much more likely to create long term instability [3].
Symptoms: Patient may have inability to walk or have anterior ankle pain.
Physical Exam: External rotation test: pain with slight dorsiflexion and external rotation. Positive tib/fib “Squeeze Test.” Talar Tilt Test: > 3 mm on Talar Tilt. Ability to hop on affected foot, lack of pain at syndesmosis, and negative external rotation tests are highly sensitive for ruling out syndesmosis injury [2].
Diagnostic Imaging: Look for > 5 mm increase in medial clear space or > 6 mm widening of tibiofibular space. Of note, plain films may only detect up 50% on AP and 66% on Mortise Views [4].
Treatment: Boot immobilization and non weight-bearing until follow up with orthopedics or sports medicine in 1 week.

Figure 2: High ankle sprain. Note the widened tibiofibular clear space. Case courtesy of RMH Core Conditions, Radiopaedia.org
Epidemiology/Importance: Most common isolated ankle fracture [5].
Symptoms: Tenderness to palpation at the lateral aspect of the ankle
Physical Exam: Most likely will be tender to palpation at lateral aspect. Make sure to check for signs of instability as above.
Diagnostic Imaging: Standard AP, Lateral, Mortise views will demonstrate fracture or unstable mortise. Consider stress view to assess for widening of tibiofibular space or medial space clearing.
Treatment:
- Weber A: Fracture below tibiotalar joint. Apply short leg walking boot and weight bearing as tolerated.
- Weber B or C: fracture at or above tibiotalar joint line. Apply short leg walking splint, non weight-bearing, and follow up in 1 week.
- Pearl: Management of Weber B fractures is institution dependent. Some institutions recommend a stress view. If normal, patients can be made weight-bearing as tolerated.
- Pearl: “Bi” or “Tri” fractures (ie. two or three malleoli fractures are identified) are always unstable. Place in a posterior leg splint with stirrup, non weight-bearing, and follow up with orthopedics. Consider ED consultation for any unstable ankle that is not amenable to splinting.

Figure 3: A) Weber A fracture, below tibiotalar joint. Case courtesy of A.Prof Frank Gaillard, Radiopaedia.org B) Weber B fracture, at tibiotalar joint. Case courtesy of Dr Alborz Jahangiri, Radiopaedia.org C) Weber C fracture, above tibiotalar joint Case courtesy of Radswiki, Radiopaedia.org
Epidemiology/Importance: Commonly missed associated fracture
Symptoms: Patient may not complain of fibular pain until palpation
Physical Exam: Tenderness to palpation anywhere along fibula
Diagnostic Imaging: Dedicated tibia/fibula x-ray will demonstrate fibular involvement
Treatment: Posterior long leg splint
- Pearl: If there is widening of the medial clear space on ankle x-ray but no other injury, strongly consider obtaining a tibia/fibula x-ray.

Figure 4: Maisonneuve fracture seen only on tib/fib view. Case courtesy of Dr Roberto Schubert, Radiopaedia.org
Epidemiology/importance: These injuries run a high risk of nonunion and avascular necrosis. Lateral process fractures have a high association with snowboarding [2]. Talar neck fractures are often associated with axial loading.
Symptoms: Patients may report lateral ankle pain.
Physical Exam: Point tenderness over lateral process near anterior talofibular ligament.
Diagnostic Imaging: Best seen on ankle mortise view. Avulsion and comminuted fractures can also be seen on lateral [2].
Treatment: Posterior short leg splint, non weight bearing, close orthopedics follow up

Figure 5: Talus fracture. Case courtesy of RMH Core Conditions, Radiopaedia.org
Epidemiology/Importance: Most frequently fractured tarsal bone [2]. Most common mechanism is fall from height. High risk to have concomitant spinal fractures.
Symptoms: Patient may have pain at heel.
Physical Exam: Palpate using heels of both hands and compressing rather than using a finger to press on certain areas.
Diagnostic Imaging: Perform Calcaneus films and measure Bohler’s Angle. If Bohler’s angle < 25 degrees, this is 100% sensitive for fracture [2]. Consider a CT if there is a high index of suspicion regardless of x-ray results.
Treatment: Posterior splint, Non weight-bearing.
- Pearl: Up to 10% of calcaneus fractures can have associated compartment syndrome of foot.

Figure 6: Calcaneus fracture. Case courtesy of Radswiki, Radiopaedia.org
Epidemiology/Importance: Typically caused by direct blow or axial loading [1]. High risk of avascular necrosis [1].
Symptoms: Vague pain and swelling at midfoot.
Physical Exam: Tenderness and ecchymosis around navicular bone [1]. May also see edema at midfoot near the navicular bone. Patients usually have full range of motion at ankle.
Diagnostic Imaging: AP, Lateral, and Oblique foot x-rays. Consider a CT if there is a high index of suspicion; plain films are only 33% sensitive for navicular fractures [2].
Treatment: Non weight-bearing, placement of posterior short leg or CAM boot and follow up with orthopedics.

Figure 7: Navicular fracture. Case courtesy of Dr Henry Knipe, Radiopaedia.org
Epidemiology/Importance: 20% are missed on initial ED presentation [6]. Typically a high energy injury such as MVC. Typically occurs when an axial load is applied to a plantar flexed foot (ie. gas pedal in MVC).
Symptoms: Pain or swelling at midfoot. Patient typically has inability to bear weight [2].
Physical Exam: Pain with torsion of midfoot (aka midfoot stress test) [Wedmore]. Ecchymosis at base of foot, especially between 2nd and 3rd metatarsal.
Diagnostic Imaging: AP, lateral, oblique foot x-ray. The base of the metatarsals should line up with the cuboids/cuneiform.
- Pearl: Consider weight-bearing foot x-ray or CT if a strong index of suspicion remains after negative plain films.
Treatment:
- If < 1 mm displacement, place in posterior short leg splint, non weight-bearing, and follow up with orthopedics within 1 week.
- If displaced, the joint is unstable and needs reduction. There is high risk for compartment syndrome.
- Pearl: Make sure to feel for the DP pulse as this injury is high risk for vascular damage.
Check out CoreEM’s post on lisfranc injuries for more information.

Figure 8: Lisfranc injury. Case courtesy of Radswiki, Radiopaedia.org
Epidemiology/Importance: Commonly missed fracture. Further classification:
- Zone 1 (Pseudo-Jones or avulsion fracture): Proximal to 4-5th metatarsal articulation
- Zone 2 (Jones fracture): Involves 4-5th metatarsal articulation
- Zone 3 (Stress fracture) : Distal to 4-5th metatarsal articulation
- Pearl: Zone 2 and 3 fractures have high risk of malunion.
Symptoms: Pain with weight-bearing over lateral border of foot
Physical Exam: Tenderness at base of 5th metatarsal
Diagnostic X-Ray: AP, Lateral Oblique foot x-rays.
Treatment:
- Zone 1 or Pseudo-Jones can be placed in CAM boot or stiff shoe and weight bearing as tolerated.
- Zone 2 and 3 fractures should be non weight-bearing, placed in CAM boot or posterior short leg splint

Figure 9: Dotted line: 4th-5th metatarsal articulation. Solid line: fracture. A) Zone 1, Pseudo-Jones fracture. Case courtesy of A.Prof Frank Gaillard, Radiopaedia.org B) Zone 2, Jones Fracture. Case courtesy of Dr Varun Babu, Radiopaedia.org C) Zone 3, Stress fracture. Case courtesy of Dr Tim Luijkx, Radiopaedia.org.
Want a basic x-ray interpretation approach to traumatic ankle imaging?
Want a basic x-ray interpretation approach to the traumatic foot imaging?
Other radiology resources
First things first: always make sure to do a thorough ankle exam.
Check out Radiopaedia’s approach to the ankle x-ray.
Don’t Forget the Bubbles has a great post on their approach and pediatric considerations.
StartRadiology has a more comprehensive approach to the ankle.
References
- Handel et al. Chapter 273. Ankle Injuries. In: Tintinalli’s Emergency Medicine. A Comprehensive Guide, 8th edition. New York: McGraw-Hill Education, 2016.
- Wedmore, I. et al. Emergency Department evaluation and management of foot and ankle pain. Emerg Med Clin N Am 33. Issue 2. May 2015. PMID: 25892727
- Hunt et al. High Ankle Sprains and Syndesmotic Injuries in Athletes. J AM Acad Ortop Surg. Vol 23. No 11. November 2015. PMID: 26498585
- Kellet, J. et al. Diagnostic imaging of ankle syndesmosis injuries: A general review. J Med Imaging Radiat Oncol. Vol 62. No 2, April 2018. PMID: 29399975
- Aiyer, AA et al. Management of Isolated Lateral Malleolus Fractures. J Am Acad Orthop Surg. Vol 27. No 2, January 2019. PMID: 30278012
- Englanoff, G. et al. Lisfranc fracture-dislocation: A frequently missed diagnosis in the ED. Annals of Emergency Medicine. Volume 26, Issue 2. August 1995. PMID 7618790

Stephen Villa, MD
Department of Emergency Medicine
University of California, Los Angeles
Latest posts by Stephen Villa, MD (see all)
- EMRad: Radiologic Approach to the Traumatic Hip/Pelvis - September 1, 2021
- EMRad: Can’t Miss Pediatric Elbow Injuries - April 5, 2021
- EMRad: Radiologic Approach to the Pediatric Traumatic Elbow X-ray - March 19, 2021


{kind=link}
{kind=link}
{kind=link}