
Sternoclavicular Joint Dislocations: Diagnosis and Treatment
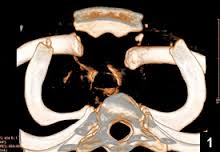
A 16-year-old football player presents to the emergency department directly from a game. He was tackled, falling onto his right shoulder. The patient is complaining of right-sided chest pain. On exam, there is tenderness over the right sternoclavicular joint (SCJ) with a prominent medial clavicle. Range of motion is limited in the right arm. What diagnostic studies need to be performed? What treatment is warranted in the emergency department?
(more…) Clinical Toxicology has published guidelines for out-of-hospital management of 16 distinct overdoses and their dose thresholds, above which, pediatric patients should be referred to the Emergency Department for evaluation. Clinical Toxicology is the official journal of the American Academy of Clinical Toxicology (AACT,
Clinical Toxicology has published guidelines for out-of-hospital management of 16 distinct overdoses and their dose thresholds, above which, pediatric patients should be referred to the Emergency Department for evaluation. Clinical Toxicology is the official journal of the American Academy of Clinical Toxicology (AACT,  Intravenous (IV) rapid sequence intubation (RSI) is by most considered the gold standard practice for securing an airway in the critically ill. There are, however, scenarios where it may not be possible to get rapid IV access in a timely manner (i.e. severe cutaneous burns, hemorrhagic shock, IV drug users, and/or the morbidly obese). It has been reported that
Intravenous (IV) rapid sequence intubation (RSI) is by most considered the gold standard practice for securing an airway in the critically ill. There are, however, scenarios where it may not be possible to get rapid IV access in a timely manner (i.e. severe cutaneous burns, hemorrhagic shock, IV drug users, and/or the morbidly obese). It has been reported that 

 Local anesthetics (LAs) are widely employed to achieve tissue infiltration, peripheral and regional anesthesia, and neuraxial blockades. Despite their well-established toxic dose limits, these agents continue to pose a substantial risk of morbidity and mortality due to local anesthetic toxicity and overdose.
Local anesthetics (LAs) are widely employed to achieve tissue infiltration, peripheral and regional anesthesia, and neuraxial blockades. Despite their well-established toxic dose limits, these agents continue to pose a substantial risk of morbidity and mortality due to local anesthetic toxicity and overdose.