
Trick of the Trade: "Pour some sugar on me" | Reducing a rectal prolapse
 Rectal prolapses are typically caused by weakened rectal muscles, continued straining, stresses during childbirth, weakened ligaments, or neurological deficits.
Rectal prolapses are typically caused by weakened rectal muscles, continued straining, stresses during childbirth, weakened ligaments, or neurological deficits.
How do you fix them? You can attempt manual reduction of the prolapse by using direct pressure. On the other extreme, corrective surgery can be performed from either an abdominal or perineal approach.
Trick of the Trade: Pour some sugar on it.
Def Leppard may have been right. Rectal prolapses often are associated with quite a bit of rectal mucosal edema. Sprinkle granulated sugar onto the area. Wait 15 minutes. The sugar reduces the edema by osmotically drawing out the fluid. The prolapse often reduces spontaneously or with gentle manual pressure.
References
- Ramanujam PS, Venkatesh KS. Management of acute incarcerated rectal prolapse. Dis Colon Rectum. Dec 1992;35(12):1154-6.
- Coburn WM III, Russell MA, Hofstetter WL. Sucrose as an aid to manual reduction of incarcerated rectal prolapse. Ann Emerg Med. Sep 1997;30(3):347-9.
 How do you risk-stratify undifferentiated chest pain patients in the Emergency Department? There are a multitude of causes for chest pain. We are always taught to think of the 5 big life-threats: ACS, PE, aortic dissection, tension pneumothorax, and pericardial tamponade.
How do you risk-stratify undifferentiated chest pain patients in the Emergency Department? There are a multitude of causes for chest pain. We are always taught to think of the 5 big life-threats: ACS, PE, aortic dissection, tension pneumothorax, and pericardial tamponade.
 From time to time, our patients need moderated and deep sedation in order to tolerate painful procedures such as joint reductions or incision and drainage procedures. There are many medications available to us including some newer ones such as Ketofol and Dexmedetomidine.
From time to time, our patients need moderated and deep sedation in order to tolerate painful procedures such as joint reductions or incision and drainage procedures. There are many medications available to us including some newer ones such as Ketofol and Dexmedetomidine.
 Have you heard of the Modified Centor Score for strep pharyngitis? Interestingly, it has been validated in adults and children. The methodology builds on the traditional Centor Score by incorporating the patient’s age, because this disease is more prevalent in kids than adults. In fact, you actually lose a scoring point if you are older than 44 years old.
Have you heard of the Modified Centor Score for strep pharyngitis? Interestingly, it has been validated in adults and children. The methodology builds on the traditional Centor Score by incorporating the patient’s age, because this disease is more prevalent in kids than adults. In fact, you actually lose a scoring point if you are older than 44 years old.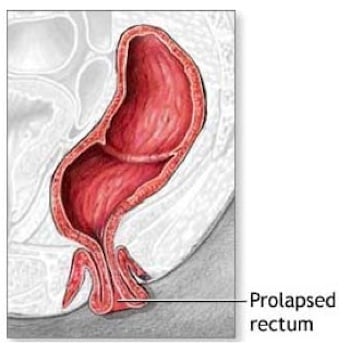{kind=link}