
Prochlorperazine, Metoclopramide, and Diphenhydramine for Acute Migraine Headache

The 2016 American Headache Society (AHS) released recommendations on managing adults with acute migraine headaches.1 In the November 2017 EM:RAP LIN Sessions podcast episode that I recorded, I realized that I overgeneralized several statements about anti-dopaminergic agents and the use of concurrent diphenhydramine for akathisia risk reduction. So I wanted to clarify things and share a deeper-dive on the topic, thanks to the constructive feedback and help of headache guru Dr. David Vinson and EM pharmacists Dr. Curtis Geier, Dr. Bryan Hayes, and Dr. Zlatan Coralic. Below summarizes the nuanced thought processes in the anti-dopaminergic treatment of migraines.

 Hurricane Maria ravaged Puerto Rico almost 3 months ago, destroying factories that manufacture and distribute medications and related supplies. Healthcare facilities across the nation are now experiencing a critical shortage of small-volume intravenous (IV) fluids, which impacts the supply of IV antimicrobials. With no end in sight, ED providers can protect the quality of patient care by considering 2 strategies: IV to PO conversion and first-dose antimicrobials via IV push.
Hurricane Maria ravaged Puerto Rico almost 3 months ago, destroying factories that manufacture and distribute medications and related supplies. Healthcare facilities across the nation are now experiencing a critical shortage of small-volume intravenous (IV) fluids, which impacts the supply of IV antimicrobials. With no end in sight, ED providers can protect the quality of patient care by considering 2 strategies: IV to PO conversion and first-dose antimicrobials via IV push.

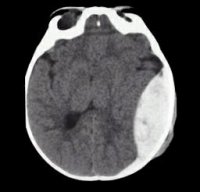 Robust and comprehensive studies now support specific management guidelines for patients presenting with different intracranial hemorrhages (ICH). From the Emergency Department perspective, the primary dilemmas involve specific blood pressure goals and whether seizure prophylaxis with phenytoin is necessary. The
Robust and comprehensive studies now support specific management guidelines for patients presenting with different intracranial hemorrhages (ICH). From the Emergency Department perspective, the primary dilemmas involve specific blood pressure goals and whether seizure prophylaxis with phenytoin is necessary. The