

Do you belong to a listserv? My favorites
An email mailing list (or listserv) is a great way to communicate with a large group of people. Once you subscribe to a mailing list, an email sent to a single, common email address will be distributed to everyone who is subscribed to the list. You can find lists for nearly everything and anything! There are a multitude of lists for various medical specialties. These lists unite people from all over the country (and world) from various practice backgrounds such as academic/community medical centers to rural hospitals/clinics. We are all connected by the power of the internet. The lists are [+]

New guest blogger: Fred Wu!
Welcome to our new superstar guest blogger, Fred Wu. Today’s post is his first (of hopefully many). Fred is the Lead PA in the Department of Emergency Medicine at Kaweah Delta Medical Center in Visalia, CA. After graduating in 2004, he has been practicing community emergency medicine in Central California. His interests include prehospital care and wilderness medicine, with an education emphasis in both. He also coordinates PA/NP training in the department as well as an EM lecture series, which hosts guest speakers from across the country. [+]

Trick of the Trade: Burned fingertips as a clinical clue
A patient presents to your Emergency Department with altered mental status and somnolence. You don’t smell alcohol on breath and you don’t see needle track marks. What clinical clue points you towards cocaine or methamphetamine ingestion? [+]

New favorite blog: Wishful thinking in medical education
Wishful Thinking in Medical Education I recently came upon this great blog by Dr. Anne Marie Cunningham, a general practitioner and Clinical Lecturer at Wales, UK. She has some really insightful posts about education, its future, and the use of new technologies. This blog has been in existence since 2008. Just as interesting are the tons of comments that she gets from a spectrum of readers. Check it out! She is also extremely active on Twitter with over 2,000 followers (@amcunningham).

Article Review: Student documentation in the chart
Do you have medical students rotating in your Emergency Department? Are they allowed to document in the medical record? Charting in the medical record is the cornerstone of clinical communication. You document your findings, your clinical reasoning, and management plan. The medical record allows communication amongst providers. Chart documentation is a crucial skill that every medical student should know, as stated by the Association of American Medical Colleges (AAMC). [+]

Paucis Verbis card: Pertussis
Is your Emergency Department administering Tdap immunization boosters instead of dT boosters? Patients with wounds are getting updated not only for tetanus and diphtheria, but also now for pertussis. Apparently there has been sharp rise in the national incidence of pertussis (Bordetella pertussis shown in image) in 2010. The infection has been documented in both infants (underimmunized less than 3 months old) and adolescents/adults (loss of immunity after 10 years). In fact, the CDC has issued an epidemic warning in California. How do you diagnose pertussis ? What are the classic symptoms? Better yet, how do you rule-it out clinically? You won't like [+]
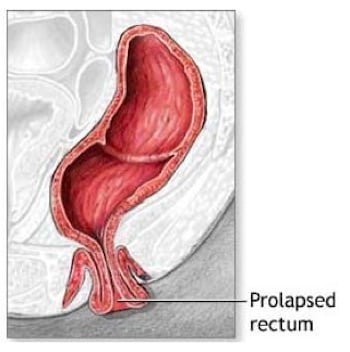
Trick of the Trade: "Pour some sugar on me" | Reducing a rectal prolapse
Rectal prolapses are typically caused by weakened rectal muscles, continued straining, stresses during childbirth, weakened ligaments, or neurological deficits. How do you fix them? You can attempt manual reduction of the prolapse by using direct pressure. On the other extreme, corrective surgery can be performed from either an abdominal or perineal approach. Trick of the Trade: Pour some sugar on it. Def Leppard may have been right. Rectal prolapses often are associated with quite a bit of rectal mucosal edema. Sprinkle granulated sugar onto the area. Wait 15 minutes. The sugar reduces the edema by osmotically drawing out the fluid. [+]

Getting a subpoena: What is an expert witness?
Well, it’s an inevitable part of working in an Emergency Department. I got a subpoena recently and now have to go in to testify on a trauma patient. I’ve gotten a few subpoenas before on trauma patients, but fortunately most cases were settled out of court. First of all, I think it’s an ethical responsibility of emergency physicians to describe what we saw and did in the care of the injured patient in the legal system. However, I have found that the few lawyers I have interacted with slowly expand their scope of questions to cover things NOT in the [+]

Article Review: Rethinking the premed requirements
Think back to your college years. Remember those premed courses that you had to take? Biology, chemistry, physics… oh my. How helpful were these in your preparation for medical school and clinical practice? In 1981, the Association of American Medical Colleges assembled a group, the General Professional Education of the Physician and College Preparation for Medicine (GPEP) to relook at these premed requirements. In 1984, the published a report “Physicians for the Twenty-First Century”. They advocated that the intensive premed requirements overly skews students’ education towards a “narrow objective of medical school admission”. Education is not balanced to include broader [+]
Paucis Verbis card: TIMI risk score
How do you risk-stratify undifferentiated chest pain patients in the Emergency Department? There are a multitude of causes for chest pain. We are always taught to think of the 5 big life-threats: ACS, PE, aortic dissection, tension pneumothorax, and pericardial tamponade. So how do YOU risk-stratify your patients for unstable angina (UA) and non-ST elevation myocardial infarction (NSTEMI)? STEMI's are usually obvious. UA and NSTEMIs -- not so much. Fortunately a 2000 JAMA article and a followup Academic Emergency Medicine 2006 study have solidified the TIMI risk scoring system as a reasonable risk-stratification tool for all-comer ED patients with chest [+]